Chapter 28: Skin Disorders
Chapter 28: Skin Disorders. Skin Lesions Defined. Skin pigment - melanin Variations may be due to anatomic, physiologic or pathophysiologic changes in skin blood flow Normal skin appearance Altered by external and internal factors Cellulitis Infectious inflammation of deep skin structures.

Chapter 28: Skin Disorders
E N D
Presentation Transcript
Skin Lesions Defined • Skin pigment - melanin • Variations may be due to anatomic, physiologic or pathophysiologic changes in skin blood flow • Normal skin appearance • Altered by external and internal factors • Cellulitis • Infectious inflammation of deep skin structures
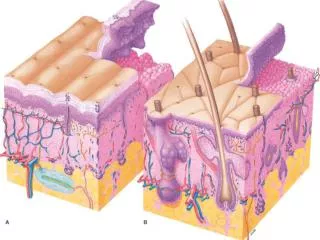
Skin Trauma • Mechanical Forces that Cause Injury • Friction • Compression • Shearing • Stretching • Scraping • Tearing • Avulsing • Puncturing
Friction and Pressure Problems • Hyperkeratosis of the Hands and Feet • Etiology • Friction and pressure over bony protuberances • Painful when subcutaneous fat becomes inelastic • Prevention • Cushioning devices; wearing 2 socks • Lubricants to reduce friction, shaving calluses • For calluses on hands, special gloves or protective gear
Sign and Symptoms • Thickening, of horny layer of skin, ovular, elongated and brown • Painful with pressure • Management • Avoid emery boards and pumice as the increase in friction will stimulate skin to produce added callus • Use moisturizer • Pair off callus with scalpel • Padding
Blisters • Etiology • Result of a shearing force that produces a raised area that accumulates with fluid • Prevention • Use of dust or powder or lubricant to reduce friction • Tubular socks, 2 pairs of socks if feet are sensitive or perspire excessively • Appropriate shoes that are broken in • Padding and lubricants • Signs and Symptoms • Hot spot, sharp burning sensation, painful • Superficial area of skin raised with clear fluid
Management (intact blister) • Leave intact for 24 hours • Clean with antiseptic • Cut small incision to drain fluid (large enough that it won’t re-seal) • Note in some states this is considered a surgical technique, placing ATC in violation of certain practice acts • Prevent refilling with a pressure pad • Clean again with antiseptic • Use doughnut to prevent irritation • Monitor for infection, replace wet bandaging • Debridement can be performed when tenderness is gone
Management (open/torn blister) • Keep clean to avoid infection • Keep skin in place and apply non-adhering sterile dressing and padding • Monitor daily for infection • Management (denuded blister) • If blister is torn 1/2 inch or more remove skin flap • Clean and expose area, apply antiseptic with occlusive dressing • Second skin can be applied to raw area
Soft Corns and Hard Corns • Etiology • Caused by pressure of improperly fitting shoes and anatomic abnormalities • Soft corns are the result of pressure and perspiration, also associated with exostosis • Signs and Symptoms • Hard corns form on the tops of toes and tend to be painful and dry • Soft corns result in thickening of skin, white and sometimes painful (between 4th and 5th toes) • Prevention • Wear properly fitting shoes • Management • Surgical removal if painful • Padding; maintain clean dry feet; wear appropriate shoes
Excessive Perspiration (hyperhidrosis) • Etiology • Syrup-like perspiration, high in sodium chloride • Increases risk of other skin irritation • Makes adherence of bandages difficulty • Management • Use of astringent such as alcohol or an absorbent powder • Aluminum chloride or electric current can be used to treat condition
Chafing of Skin • Etiology • Occurs particularly in athletes that are obese or heavy limbed • Result of friction and maceration of skin in climate of heat and moisture • Signs and Symptoms • Separation of keratin from granular layer of skin • Causes oozing wounds that crust and crack • Prevention • Keep skin dry, clean, and friction free • For the groin, soft, loose, cotton underwear is recommended • Management • Clean area with soap and water and treat with medicated solution and hydrocortisone cream
Xerotic (Dry) Skin • Etiology • Drying of skin due to exposure of cold, excessive bathing, decrease in humidity causing skin to lose water • Signs and Symptoms • Dry skin w/ variable redness and scaling; itching • Management • Prevent water loss and replace lost water • Bathe in tepid water, use moisturizer • If condition worsens, refer to physician
Ingrown Toenails • Etiology • Generally occurs in great toe • Nail grows laterally into skin • Result of lateral pressure from shoes, poor nail trimming, and repeated trauma
Signs and Symptoms • Pain and swelling • Penetrated skin becomes inflamed and purulent with lateral nail fold swollen and irritated • Prevention • Properly fitting shoes and socks are essential • Weekly toenail trimming (cut straight across) • Leave nail long enough to clear skin • Management • Conservative management includes soaking the inflamed toe in warm water (20 minutes) • Place cotton under edge of nail to clear from skin • If chronic, remove wedge of nail and apply antiseptic compress until inflammation resides • Physician may take more aggressive approach
Wounds • Abrasions • Scraping of skin against rough surface (top surface of skin is worn away) • Increased probability of infection due to exposure of dirt and foreign material • Clean and debride • Punctures • Direct penetration of skin with pointed object • Must be referred to physician
Lacerations • Object tears tissue, giving wound appearance of jagged edge (sometimes result of blunt trauma) • Presents environment susceptible to infection • Skin Incision • Smooth cut in skin - not jagged • Skin Avulsion • Skin torn away from body (should be placed in moist gauze w/in a plastic bag that is then immersed in cold water) • Transport to hospital with athlete for possible reattachment
Skin Bruises • Result of blunt trauma; causes disruption of superficial blood vessels and results in black and blue discoloration • Treatment requires RICE to control hemorrhaging
Wound Management • All wounds must be assumed contaminated • Pay close attention to all universal precautions • Clean all wounds with soap and water to minimize infection • Apply a dressing with antiseptic (unless physician examination is necessary) • Lacerations and punctures should be treated by a physician • Use of occlusive dressings • Minimizes scab formation, perceived pain from exposed nerves, cost and time effective, provide adequate barrier • Antibiotic ointment used to prevent secondary infection (SEE TABLE 28-4 for added instruction)
If the wound is discharging serum (fluid) to dressing should be changed regularly • When drainage has stopped = no need for dressing • Wound should be cleaned with hydrogen peroxide or Betadine • Effective against bacteria and not harmful to fibroblasts • Antibacterial ointment should be used to limit bacterial growth and to prevent dressing from adhering to wound • Proper care = minimized inflammatory response with quick healing and reduced scarring
Suturing • Dependent on severity • Determined by physician • Should be put in as soon as possible • Within 12 hours following injury • Utilize fine suture material and minimal tightening • Limits additional damage, inflammation and scarring • Large areas or slow healing areas = larger material to be left in longer • Occasionally steri-strips or butterfly bandages will suffice
Athletic Training Room Practice in Wound Care • Use clean and sterile instruments • Clean hands thoroughly and use gloves • Clean in and around skin lesion • Use a non-medicated covering if athlete is to be sent for medical attention • Avoid touching any part of sterile dressings that will contact the wound • Place medication on pad • Secure the dressing in place
Bacterial Infections • Bacteria are single celled micro-organisms • Spherical, doublets, and spirochetes • Staphylococcus • Gram positive bacteria that appears in clumps in skin and upper respiratory tract • Streptococcus • Chain bacteria often associated with systemic disease and skin infections • Bacillus • Spore forming, aerobic, and occasionally mobile • Can cause systemic damage
Impetigo Contagiosa • Etiology • Caused by A-beta-hemolytic streptococci, S aureus or combination of these bacteria • Spread through close contact • Signs and Symptoms • Mild itching and soreness followed by eruption of small vesicles and pustules that rupture and crust • Generally develops in body folds that are subject to friction • Management • Cleansing and topical antibacterial agents • Systemic antibiotics
Furunculosis (Boils) • Etiology • Infection of hair follicle that results in pustule formation • Generally the result of a staph. infection
Signs and Symptoms • Pustule that becomes reddened and enlarged as well as hard from internal pressure • Pain and tenderness increase with pressure • Most will mature and rupture • Management • Care involves protection from additional irritation • Referral to physician for antibiotics • Keep athlete from contact with other team members while boil is draining
Carbuncles • Etiology • Similar in terms of early stage development as furuncles • Signs and Symptoms • Larger and deeper than furuncle and has several openings in the skin • May produce fever and elevation of WBC count • Starts hard and red and over a few days emerges into a lesion that discharges yellowish pus • Management • Surgical drainage combined with the administration of antibiotics • Warm compress is applied to promote circulation
Folliculitis • Etiology • Inflammation of hair follicle • Caused by non-infectious or infectious agents • Moist warm environment and mechanical occlusion contribute to condition • Psuedofolliculitis (PFB)
Signs and Symptoms • Redness around follicle that is followed by development of papule or pustule at the hair follicle • Followed by development of crust that sloughs off with the hair • Deeper infection may cause scarring and alopecia in that area • Management • Management is much like impetigo • Moist heat is used to increase circulation • Antibiotics can also be used depending on the condition
Hidradenitis Suppurativa • Etiology • Primary inflammation event of the hair follicle resulting in secondary blockage of the apocrine gland • Signs and Symptoms • Begins as small papule that can develop into deep dermal inflammation • Management • Avoid use of antiperspirants, deodorants and shaving creams • Use medicated soaps and systemic antibiotics
Acne Vulgaris • Etiology • Inflammatory disease of the hair follicle and the sebaceous glands • Sex hormones may contribute • Signs and Symptoms • Present with whiteheads, blackheads, flesh or red colored papules, pustules or cysts • If chronic and deep = may scar • Psychological impact • Management • Topical and systemic agents used to treat acne • Sometimes the use endogenous hormones is required • Mild soaps are recommended
Paronychia and Onychia • Etiology • Caused by staph, strep and or fungal organisms that accompany contamination of open wounds or hangnails • Damage to cuticle puts finger at risk • Signs and Symptoms • Rapid onset; painful with bright red swelling of proximal and lateral fold of nail • Accumulation of purulent material w/in nail fold • Management • Soak finger or toe in hot solution of Epsom salt 3 times daily • Topical antibiotics, systemic antibiotics if severe • May require pus removal through skin incision
Tetanus Infection (lockjaw) • Etiology • Acute infection of the CNS caused by tetanus bacillus • Bacteria enters through the blood and open wounds • Signs and Symptoms • Stiffness of the jaw and muscles of the neck • Muscles of facial expression produce contortion and become painful • Fever may become markedly elevated • Management • Treat in intensive care unit • Childhood immunization
Fungal Infections • Group of organisms that include yeast and molds which are usually not pathogenic • Grow best in unsanitary conditions with warmth, moisture and darkness • Infections generally occur in keratinized tissue found in hair, nails and stratum corneum • Dermatophytes (Ringworm fungi) • Cause of most skin, nail and hair fungal infections
Tinea of the Scalp (tinea capitis) • Signs and Symptoms • Ringworm of the scalp begins as a small papule that spreads peripherally • Appears as small grayish scales resulting in scattered balding • Easily spread through close physical contact • Management • Topical creams and shampoos are ineffective in treating fungus in hair shaft • Systemic antifungal agents are replacing older agents due to increased resistance • Some topical agents are used in conjunction
Tinea of the Body (tinea corporis) • Signs and Symptoms • Commonly involve extremities and trunk • Itchy red-brown scaling annular plaque that expands peripherally • Management • Topical antifungal cream
Tinea of the Nail (tinea unguium/ onchomycosis) • Signs and Symptoms • Fungal infection of the nail -- found commonly in those engaged in water sports or who have chronic athlete’s foot • Nail becomes thick, brittle and separated from its bed • Management • Some topical antifungal agents have proved useful • Systemic medications are most effective • Surgical removal of nail may be necessary if extremely infected
Tinea of the Groin (tinea cruris) • Etiology • Symmetric red-brown scaling plaque with snake-like border • Signs and Symptoms • Mild to moderate itching
Management • Treat until cured • Will respond to many of the non-prescription medications • Medications that mask symptoms should be avoided • Failure to respond to normal management may suggest a non-fungal problem (such as bacteria) and should be referred to a physician • May require additional topical medications and oral prescriptions
Athlete’s Foot (tinea pedis) • Etiology • Most common form of superficial fungal infection • Tricophyton species are most common cause of athlete’s foot • Webs of toes may become infected by a combination of yeast and dermatophytes • Signs and Symptoms • Extreme itching on soles of feet, between and on top of toes • Appears as dry scaling patch or inflammatory scaling red papules forming larger plaques • May develop secondary infection from itching and bacteria • Management • Topical antifungal agents and good foot hygiene
Candidiasis (Moniliasis) • Etiology • Yeast-like fungus that can produce skin, mucous membrane and internal infections • Ideal environment includes hot humid weather, tight clothing, and poor hygiene • Signs and Symptom • Infections w/in body folds • Presents as beefy red patches and possible satellite pustules • White, macerated border may surround the red area; deep painful fissures may develop at skin creases • Management • Maintain dry area • Use antifungal agents to clear infection
Tinea Versicolor • Etiology • Caused by a yeast • Appears commonly in areas in which sebaceous glands actively secrete body oils • Signs and Symptoms • Fungus produces multiple, small, circular macules that are pink, brown, or white • Commonly occur on chest, abdomen, and neck • Do not tan when exposed to sun and usually are asymptomatic • Management • Straightforward treatment - recurrences are common • Use selenium shampoo (Selsun) and topical econazole nitrate (or something similar) • When microorganism has been eradicated, re-pigmentation of the area will occur