Download
1 / 58
580 likes | 597 Vues
Learn about transtracheal ventilation as a last resort in airway emergencies, the principle of Venturi system adaptation, and existing devices for manual jet ventilation.

E N D
Transtracheal Lung Ventilation using a Manual Respiration Valve -Not a patent - free to be produced- Dragan Pavlovic Formerly Department of Anaesthesiology, Ernst-Moritz-Arndt-University Greifswald, Germany Conflict of interests: Dragan Pavlovic and Michael Wendt. A Device for Manual Ventury-Jet Ventilation, German Patent Office N° 202.13.420.2 (August 29, 2002 – EXPIRED in 2012) and Dragan Pavlovic, German Patent Office Nr.: 10 2009 029 959.9 (23.06.2009).
“Can not intubate, can not ventilate”: transtracheal ventilation Practice guidelines for management of the difficult airway: an updated report by the American Society of Anesthesiologists Task Force on Management of the Difficult Airway. Anesthesiology 2003; 98 (5): 1269-77. Airway Management. Leitlinie der Deutschen Gesellschaft für Anästhesiologie und Intensivmedizin. Anaesth Intensivmed 2004; 45: 302-306. Recommendations for airway control and difficult airway management. Minerva Anestesiol. 2005, 71(11):617-57. Recommendations for airway control and difficult airway management in pediatric patient. Minerva Anestesiol. 2006, 72(11):723-48.
“Can not intubate, can not ventilate”: transtracheal ventilation Background. In the extreme and rare emergency, when the patients could be neither intubated nor ventilated (“can not intubate, can not ventilate”) due to upper airway obstruction or in cases of “difficult intubation”, as the last resource, ventilation through a transtracheal cannula is attempted. Patel, R.G. Percutaneous transtracheal jet ventilation: a safe, quick, and temporary way to provide oxygenation and ventilation when conventional methods are unsuccessful. Chest. (1999), 116: 1689-94
“Can not intubate, can not ventilate”: transtracheal ventilation Lung inflation is maintained with a kind of jet ventilation while the lung empties through the upper airways (if they are open – what is not always the case) and through the trans-tracheal cannula. This is done until help is obtained and ordinary airway assured in a hospital emergency department. If the airway pressure is not monitored, to avoid hyperinflation and lung injury, it is necessary to closely observe the thorax excursions while ventilating the lungs. O2 Patel, R.G. Percutaneous transtracheal jet ventilation: a safe, quick, and temporary way to provide oxygenation and ventilation when conventional methods are unsuccessful. Chest. (1999), 116: 1689-94.
Existing Systems „Manujet“(VBM) Price: $430
Existing Systems „Manujet“
Existing Systems Enk-Set (COOK) Price: 88.50 euro Enk, D., Busse, H., Meissner, A., and Aken, H. van. A new device for oxygen and drug administration by transtracheal jet ventilation, Anesth. Analg. (1998), 86: 203. Preussler N., Schwarzkopf K., Schreiber T., et al. Ein Vergleich zwischen dem “oxygen flow modulator” und der niederfrequenten Jetventilation zur transtracheale Oxygenierung im Tiermodell. Anästhesiologie & Intensivmedizin (2001), 42: 481
Existing Systems Manual Jet Ventilator (Instrumentation Industries, Inc.) Price: $140
pulmonary pressure PEEP time Problem O2 Inspiration: very high driving pressure Transtracheal cannula= high flow resistance Expiration = low driving pressure
pulmonary pressure PEEP time Problems With the Existing Systems Major problem isupper airway obstruction – thatmay be the very cause for “can not intubate, can not ventilate”! High inspiratory flow that is followed by law, passive expiratoryflow through 1-2mm diametar trans-tracheal cannula may result in: 1. Build up of dynamic PEEP 2. Dangerous hyperinflation Low respiratory frequency that would permit lung empting will induce: 3. hypoventilation
Existing Systems Active expiration is needed for the existing systems to function properly Available devices do not have a facility for active expiration. The only available device that uses expiratory aid is a full jet ventilator with double lumen trans-tracheal tube, described by Garry B et al. (B., Garry., Woo, P., Perault, F. D., Shapshay, S., and Wurm, H.. Jet ventilation in upper airway obstruction: description and model lung testing of the new jetting device, (1998) Anesth Analg, 87: 915 – 920., US patent, US005669380, the application filed by 639,167, Apr. 26, 1996)
A solution? O2
A solution? O2
A solution? O2
A solution? O2
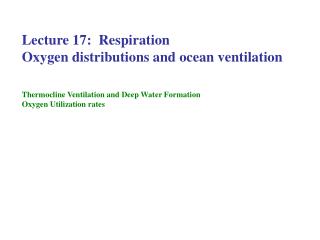
Venturi system 2.5mm 5mm 1.4mm 20mm 3mm Daniel Bernoulli 1700-1782 Giovanni Battista Venturi, (1746–1822)
GreifPump How the venturi system was addapted Principle 1 Venturi system 2.5mm 5mm 1.4mm 20mm 3mm 30mm (Dragan Pavlovic & Michael Wendt, German Patent Office, N° 202.13.420.2, August 29, 2002)
GreifPump How the venturi system was addapted Principle 2 Venturi system 2.5mm 5mm 1.4mm O2 30mm (Dragan Pavlovic & Michael Wendt, German Patent Office, N° 202.13.420.2, August 29, 2002)
GreifPump How the venturi system was addapted Principle 3 Venturi system 2.5mm To the patient 1.4mm O2 (Dragan Pavlovic & Michael Wendt, German Patent Office, N° 202.13.420.2, August 29, 2002) 30mm
GreifPump. Experimental prototype: Fabrication – metal Venturi system (Dragan Pavlovic & Michael Wendt, German Patent Office, N° 202.13.420.2, August 29, 2002)
GreifPump. Experimental prototype: Fabrication - metal Venturi system 1.5-2.0mm dihtung 7mm 4.0mm O2 2.5mm 20mm 2.0mm 3mm To patient (Dragan Pavlovic & Michael Wendt, German Patent Office, N° 202.13.420.2, August 29, 2002) 30mm
GreifPump. Experimental prototype: Fabrication - glass (Dragan Pavlovic & Michael Wendt, German Patent Office, N° 202.13.420.2, August 29, 2002)
GreifPump. How it works Functioning. Manual closure (with finger) of the outlet (c) forces gas to flow back through the side tube (d) (“inspiration”). The close-open maneuvers makes the pump functioning as a blowing-suctioning apparatus. The suctioning power is 2-3 times smaller then blowing and for moving the equal volumes in both directions, suctioning time has to be 2-3 times longer then blowing time. Our GreifPump C O2 d (Dragan Pavlovic & Michael Wendt, German Patent Office, N° 202.13.420.2, August 29, 2002) To trachea
GreifPump. How it works: Finger on: inspiration O2 O2 inspiration Cartilago thyrodidea Cartilago cricoidea trachea (Dragan Pavlovic & Michael Wendt, German Patent Office, N° 202.13.420.2, August 29, 2002)
GreifPump. How it works: Finger off (suction): facilitated expiration O2 O2 O2 Facilitated expiration Cartilago thyrodidea Cartilago cricoidea trachea (Dragan Pavlovic & Michael Wendt, German Patent Office, N° 202.13.420.2, August 29, 2002)
Experiments in vitro (test lung simulator settings) Average conditions: airway resistance (r) = 2mbar/l sec-1, respiratory system compliance (C) = 0.1 l/mbar peak inspiratory pressure (Pip) = 10mbar
RESULTS In vitro Metall venturi I:E times for 1.0 litre Vt; 16G Spontaneous expiration Flow (F) (l/min) I:E R 1000ml Inspired volume 4.0 14.8:31.4 2.12 4.3 13.7:30.6 2.23 5.4 11.1:30.5 2.74 5.6 10.7:29.3 2.74 6.8 8.8 :30.9 3.40 10.0 6.9 :22.2 3.21 14.0 4.2 :18.0 4.28 300ml 20 10 0 10 20 30 40 50 60 time (s) Vt of 300ml O2 may be sufficient for normal oxygenation Inspiratory time (*) expiratory time Pavlovic, Dragan. A Device for Manual Ventury-Jet Ventilation, German Patent Office N° 202.13.420.2, August 29, 2002
RESULTS In vitro Glass venturi I:E times for 1.0 litre Vt 16G inner diameter (about): 0.053in = 1.345mm 12G inner diameter (about): 0.089in = 2.260mm Inspiration expiration *) Inspiration time for 1.0 litre =60/F (pre-set value) 300ml Vt of 300ml O2 may be sufficient for normal oxygenation Pavlovic, D, K. Meissner, H.-E. Wagner, U. Bartels, and M. Wendt, Bi-directional Venturi Pump for Emergency Transtracheal Lung Ventilation, Intensiv Medizin und Notfallmedizin 39 (Suppl 1): 49, 2002 K. Meissner, T. I. Usichenko, Ch. Lehmann, M. Wendt and D. Pavlovic Bi-directional Venturi Pump for Short Term Emergency Transtracheal Lung Ventilation ASA 2003, San Francisco, USA.
RESULTS In vitro Glass venturi I:E times for 1.0 litre Vt 16G inner diameter (about): 0.053in = 1.345mm 12G inner diameter (about): 0.089in = 2.260mm Inspiration expiration *) Inspiration time for 1.0 litre =60/F (pre-set value) 300ml Vt of 300ml O2 may be sufficient for normal oxygenation
RESULTS In vitro Glass venturi I:E times for 1.0 litre Vt Inspiration expiration *) Inspiration time for 1.0 litre =60/F (pre-set value) 300ml The limiting factor for minute lung ventilation in very comliant lungs and with high airway resistance may be relativelly long expiratory time.
RESULTS.In vivo, pilot study(3 pigs) The GreifPump was also tested in the pigs (32-40kg. N=3) and it was concluded that it provides adequate lung ventilation if the flow of gas (100% of O2 that was used produced even extreme over-oxygenation) is over 6l/min and intratracheal cannula 16G or greater. Bellow, results of the experiment: Flow: 140ml/sec (8.4l/min), cannula 16G. mmHg Time following begunining of trans-tracheal ventilation with GreifPump
Further In-vivo Tests (5 pigs) of a Bi-directional Venturi Pump for Emergency Transtracheal Lung Ventilation Konrad Meissner, Thomas Iber, Jan-Patrick Roesner, Christian Mutz, Christina Layher, Christian Lehmann, Michael Wendt, and Dragan Pavlovic In-vivo Tests of a Bi-directional Venturi Pump for Emergency Transtracheal Lung Ventilation ESA-2005, Vienna Dragan Pavlovic, Konrad Meissner, Thomas Iber, Jan Roesner, Christian Mutz, Christina Layher, Christian Lehmann, and Michael Wendt Bi-directional venturi pump can provide satisfactory transtracheal lung ventilation during more then 1 hour in 40kg pigs HAI-2005, Berlin Konrad Meissner, Thomas Iber, Jan-Patrick Roesner, Christian Mutz, Hans-Erich Wagner, Christina Layher, Utz Bartels, Matthias Gründling, Taras I. Usichenko, Michael Wendt, Christian Lehmann, and Dragan Pavlovic Successful Transtracheal Lung Ventilation using a Manual Respiration Valve-an in vitro and in vivo Study, Anesthesiology. 2008 Aug;109(2):251-9 Animals (pigs, 40kg, n=5) were anesthetized and mechanically ventilated (tidal volume about 10 ml/kg), to be then ventilated through transtracheal 16 G cannula (while the tracheal tube was blocked) using the venturi device. Predefined inspiration times (0.8, 1.5 and 2 sec) and two different gas flows (12 and 16 l/min) were tested. In addition to blood gas analysis and the recording of arterial, pulmonary artery, central venous and tracheal pressures,continuous cardiac output measures were performed.
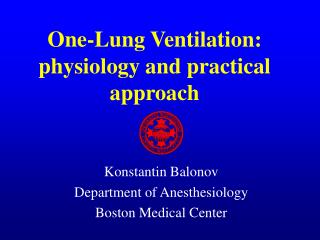
pCO2 pO2 600 500 462.5±75.3 400 300 16 l/min, I/E 0.8/4.5 sec 200 A 100 84.4±16.8 0 0 10 20 30 40 50 60 600 500 490.5±59.2 400 arterial blood partial pressures (mm Hg) 300 16 l/min, I/E 1.6/8.5 sec 200 B 100 64.9±10.0 0 0 10 20 30 40 50 60 600 500 470.8±86.8 400 300 12 l/min, I/E 2/8.5 sec 200 C 100 63.0±7.2 0 0 10 20 30 40 50 60 time (min) Results Arterial pO2 and pCO2 values for the three conditions tested (A: flow 16 l/min, I/E ratio 0.8/4.5 sec; B: flow 16 l/min, I/E 1.6/8.5 sec, C:flow 12 l/min, I/E ratio 2/8.5 sec) are given in Fig. 3. The other recorded physiologic parameters did not change significantly during venturi ventilation. The tracheal pressures (max 9.4, min 1.8 cm H2O) corresponded to central venous and pulmonary artery pressures. Cardiac output rose from 4.5±1.1 to 5.0±2.2 l/min in the high flow/high frequency experiments (A) but slightly dropped (4.9±1.0 to 3.9±1.1 (B); 5.3±0.9 to 4.1±1.1 (C)) in both low-frequency groups. Occasional PEEP increases were inversely proportional to the cardiac output. Anesthesiology. 2008 Aug;109(2):251-9 After 1 hour
RESULTS summary We found that when increasing the flow rate both inflation and deflation times shortened, but I:E ratio (R) increased and deflation time lag progressively behind inflation time, as it was predicted by the mathematical model. The less favorable conditions were modeled with C set at 0.03 l/mbar (Pip was 30mbar) when time of spontaneous lung emptying approached that achieved with the venturi pump set at F<10 l/min. Anesthesiology. 2008 Aug;109(2):251-9
Conclusions With medium gas flow of about 10l/min, and with an I:E ratio of about 1:3.5, we predicted that satisfactory ventilation of the normal adult lungs could be expected with this model. An adequate ventilation of pathological or smaller lungs (in children) would require adjustment of the flow rate and/or of I:E ratio. The performance of the venturi pump could be predicted to great extent but a calibration would be needed in order to produce tables that would recommend flow and I:E ration for the given lung volume. Anesthesiology. 2008 Aug;109(2):251-9
Use 1. This is self-contained valve that, with a supply with pressurised gas (oxygen), can provide lung insuflation by the closure of one orifice with a finger, and when orifice opened, active expiration true trans-tracheal cannula. 2. The device should be present in every emergency department and every emergency vehicle replacing devices that are in use. 3. This cheep device can be routinely added to the bottles containing medical air or oxygen to be used as a suctioning or for trans-tracheal lung ventilation in cases of emergency. 4. Visual control of thorax movement may give satisfactory insight into ventilation and, in emergency, the use of the GreifPump may be recomanded. 6. Being an emergency device its possible drawbacks (jet injury to the bronchial mucosa, no control of delivered volumes) may be largely ignored.
This device is free, the patent-like protection expired in 2012
Enk’s replica Dr.Enk changed our model probably in order to claim a patent, but weakened its Venturi effects. Enk, Dietmar. Gas flow reversing element, Deutsche Patent Office, DE 10 2007 013 385 A1 2008.09.18 or under other similar patent registrations: Enk D. Gasstromumkehrelement. Patent application (10 2007, 013 385.7). German Patent Office, March 16, 2007 WO2008113752 A3 WO2008113752 A2 CA2681121 A1 Let us have a look at the first Patent “Enk, Dietmar. Gas flow reversing element, Deutsche Patent Office, DE 10 2007 013 385” In documentation from German Patent Office is to find that this Patent was REMOVED (Nicht anhängig/erloschen)! Last registration was 30.01.2013. https://register.dpma.de/DPMAregister/pat/register?AKZ=1020070133857 or https://register.dpma.de/DPMAregister/pat/PatSchrifteneinsicht?docId=DE102007013385A1&page=1&dpi=150&lang=de We presume that the DPO removed it because it was identical with our model from 2002. However, Dr. Enk registered the SAME Patent outside of Germany (see above) probably to avoid the problem. (For how long?)
Problems of the Enk model B (Enk 2007) A (Pavlovic 2002) To lungs To lungs • The two models are the same in respect to protected characteristics of the model of Pavlovic 2002 (the protection expired in 2012). • Dr. Enk used probably larger tubing overall, but, • shortened the injector tube and • (2) pulled it backwards and • (3) prolonged the narrow part of the exit tube, replacing the conical exit tube with an • (4) equally narrow tube.
Since the Enk’s patent protects only his trivial changes of our previously protected model, THEREFORE, the device is free, since its patent-like protection expired in 2012
Perspectives • Intermittent airway pressure measurements by stop-flow at the end of expiration (at every 5-8 cycles, at the end of suctioning; currently used system do not have this facility) would assure that the lungs are at functional residual capacity (FRC) and that ventilation may be continued without danger of over-inflation. However this does not have to be included in standard equipment. • Potentially, it can be used as a jet ventilator in ORL surgery if the upper airways are obstructed, assuring complete lung emptying and removing a danger of hyperinflation that is always present when using classical jet ventilators. (Dragan Pavlovic, German Patent Office Nr.: 10 2009 029 959.9 (23.06.2009). b a O2 c d patient Preasure transducer
Perspectives (Dragan Pavlovic, German Patent Office Nr.: 10 2009 029 959.9 (23.06.2009).
Perspectives … or with variable expiratory-inspiratory flows O2 Pressure knob Security valve To manometer from patient (Dragan Pavlovic, German Patent Office Nr.: 10 2009 029 959.9 (23.06.2009).
Perspectives … or with variable expiratory-inspiratory flows O2 Pressure knob Security valve To manometer To patient (Dragan Pavlovic, German Patent Office Nr.: 10 2009 029 959.9 (23.06.2009).
Perspectives … or with variable expiratory-inspiratory flows O2 Pressure knob Security valve To manometer from patient (Dragan Pavlovic, German Patent Office Nr.: 10 2009 029 959.9 (23.06.2009).
Perspectives … or with variable expiratory-inspiratory flows O2 Pressure knob Security valve To manometer To patient (Dragan Pavlovic, German Patent Office Nr.: 10 2009 029 959.9 (23.06.2009).
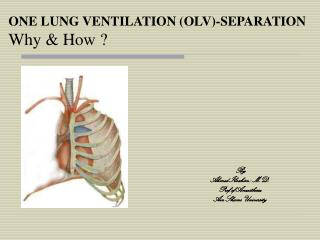
A. During inspiration, when squeezed with the hand, the outflow is blocked (while the inflow to the venturi nozzle is reduced by the action of the lower part of the handle (B). The device is hold in a hand and when sqeesed, upper and lower part (A and B) move inwards and reduce the flow (A) and close the outflow (B). O2, high pressure, about 15L/min B To the lungs A This blocks the gas inflow when moved inwards by squeezing the handle (the extent of movement should be adjustable). B. During inspiration, when squeezed with the hand, flow is reduced. (Dragan Pavlovic, German Patent Office Nr.: 10 2009 029 959.9 (23.06.2009).
From the lungs 10mm 5mm O2 7mm 2.5 mm 3mm (Dragan Pavlovic, German Patent Office Nr.: 10 2009 029 959.9 (23.06.2009).