Download
1 / 58
620 likes | 1.08k Vues
SCABIES, LICE AND HPV. Michael E. Hagensee, M.D. Ph.D. Associate Professor Department of Medicine Section of Infectious Disease LSUHSC. DISCLOSURE.

E N D
SCABIES, LICE AND HPV Michael E. Hagensee, M.D. Ph.D. Associate Professor Department of Medicine Section of Infectious Disease LSUHSC
DISCLOSURE I have no financial interests or other relationship with manufacturers of commercial products, suppliers of commercial services, or commercial supporters. My presentation will not include any discussion of the unlabeled use of a product or a product under investigational use.
STDs AND OTHER GYNECOLOGIC INFECTIONS • Objectives: • To be able to diagnose and treat scabies • To be able to diagnose and treat pubic lice • To know about the disease that HPV cause and • how to treat/prevent them
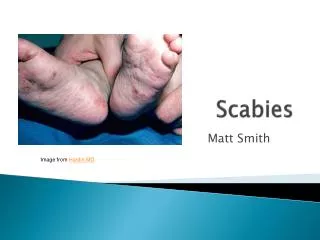
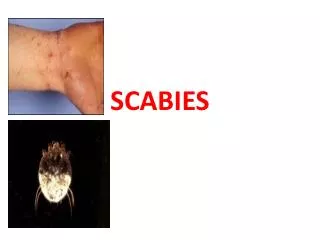
SCABIES A. Etiology:Sarcoptes scabiei-human itch mite B. Epidemiology: 1. More than 100 million cases per year 2. Itching due to excretions from burrowing mites 3. Increase spread by close contact, crowding 4. Medical practitioners are at high risk C. Clinical manifestations: 1. Itching increases at night and after a hot shower 2. Burrows-dark wavy lines ending in small bleb 3. Usual sites wrists, fingers, elbows and on penis 4. Usually 15 mites per person
SCABIES 5. Norwegian scabies: (crusted) - thousands to millions of mites per person - seen only in immunosuppressed (HIV) individuals - erythema, thick keratotic crusts and dystrophic nails D. Diagnosis: Find mite of eggs in scraping vs empiric E. Treatment: 1. 5% permethrin cream 2. 1% lindane (not in pregnant women) 3. Anti-pruritics as needed
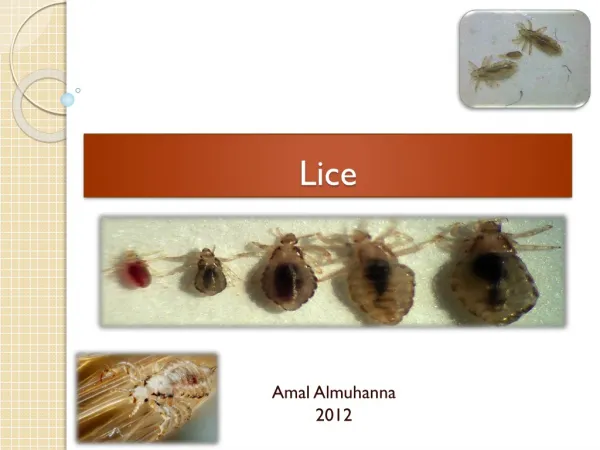
LICE A. Etiology: 1. Pediculus humanus var. capitis - head lice 2. P. humanus var. corporis - clothing 3. Pthirus pubic - pubic hair B. Epidemiology: 1. Lice feed on human blood once a day 2. Saliva of lice produce an irritating rash 3. Transmitted by close contact, shared combs, clothing
LICE C. Clinical manifestations: 1. Intensely pruritic lesions 2. 2-3 mm blue macules (maculae cerulae) at bite sites D. Diagnosis: Find nits or adult lice in hair or clothing E. Treatment: 1. 1% permethrin 2. 0.5% malathion 3. 1% lindane - more toxic and must apply a second dose 1 week later - does not kill nits - not in pregnant women 4. Comb out nits after treatment
HUMAN PAPILLOMAVIRUS (HPV) • Papovavirus • Most common viral STD • ds DNA virus of 7.9 kB • Entire DNA sequence is • known
HPV TYPES Defined by 10% difference in DNA sequence (L1 gene) • 1,2 - plantar and • common warts • 6,11 - condylomata and • laryngeal warts • 16,18, and others - • anogenital malignancies
METHODS TO DETECT HPV INFECTION Clinical diagnosis: Genital warts Epithelial defects See cellular changes caused by the virus: Pap smear screening Directly detect the virus: DNA hybridization or PCR* Detect previous infection: (Research Only) Detection of antibody against HPV* * Done in the Hagensee Laboratory
HPV EPIDEMIOLOGY GENITAL WARTS • Usually caused by HPV 6 or 11 • Prevalence has increased 2-10x over past 30 years • Most often found on penile shaft and anus in men, • vulva in women • Spontaneous regression seen in 20% of cases
GENITAL HPV INFECTION DIFFERENTIAL DIAGNOSIS • CONDYLOMA LATUM-SYPHILIS • MOLLUSCUM CONTAGIOSUM • FIBROEPITHELIOMA AND OTHER CANCERS • LICHEN PLANUS • OTHER-HSV, LGV, CHANCROID, • GRANULOMA INGUINALE
GENITAL HPV INFECTION TREATMENT • OBSERVATION -20% spontaneous regression • CRYOTHERAPY -70% cure rate • PODOPHYLLIN/ TCA -30% cure rate • SURGERY -laser-85% cure rate • INTERFERON ALPHA -intralesional and systemic • IMIQUIMOD -induces local interferon alpha production • CIMETIDINE (Tagamet) – non-specific immune booster
HPV EPIDEMIOLOGY ANOGENITAL MALIGNANCY • Caused by high risk HPVs-16, 18, 31 and others • Occurs mainly in older women-average age 54 years • Associated with increased number of sexual partners, • smoking, and immune suppression
HPV IS ASSOCIATED WITH ANOGENITAL MALIGNANCIES • HPV DNA is found in 50-98% of tumors depending • on location • Oncogenic genes (E6 and E7) of high-risk types are • expressed in tumors • E6 and E7 of high-risk types are oncogenic in-vitro • Support from many epidemiologic studies
CERVICAL CANCER CIN II
CERVICAL CANCER 2nd most common malignancy of women worldwide More than 500,000 cases per year # of cases declining in USA Over 13,000 cases in US in 1998 Over 35% mortality
COLLECTION OF A PAP SMEAR CONVENTIONAL NOW MOST CLINICS HAVE MOVED TO LIQUID-PAP SMEARS (Thin Prep, SurePath) - preserve the morphology of the cells better
HPV DIAGNOSIS – PAP SMEAR Normal, ASCUS – Atypical Squamous Cells of Unclear Significance
HPV PAP SMEARS Pap smear: Normal ASCUS – atypical cells of unclear significance: repeat Pap vs test for HPV DNA LGSIL – low grade squamous intra-epithelial lesion: colposcopy with biopsy HGSIL – high grade squamous intra-epithelial lesion: colposcopy with biopsy and treat Cervical biopsy: CIN I – mild dysplasia – usually spontaneously regresses CIN II – moderate dysplasia - treat CIN III – severe dysplasia – treat Carcinoma – in-situ – treat Invasive cervical cancer – treat
CERVICAL CANCER SCREENING METHODS • HPV DNA Testing for questionable cases: • Normal PAP smear - usual follow up • ASCUS - may be cost-effective • LGSIL - most regress • HGSIL - refer for colposcopy and biopsy
CERVICAL CANCER SCREENING METHODS REFLEX TESTING USING HYBRID CAPTURE II Collect a cervical swab for DNA testing from all women and store them Only those women with ASCUS (or LGSIL) – the swab is sent for HPV DNA testing HCII – positive for high-risk HPV – then refer to colposcopy negative for high-risk HPV – then routine yearly screening