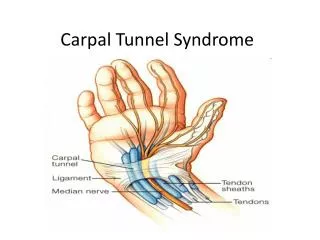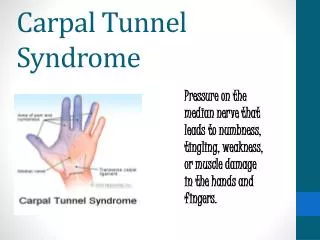
Carpal Tunnel Syndrome
180 likes | 419 Vues
Carpal Tunnel Syndrome. A New Care Pathway. Format. Introduction (5mins) SL Current Rheumatology issues (15mins) AY Current Orthopaedic Issues (10mins) ND Introduction to pathway (5mins) SL Pairs to consider pathway (10mins) ALL

Carpal Tunnel Syndrome
E N D
Presentation Transcript
Carpal Tunnel Syndrome A New Care Pathway
Format • Introduction (5mins) SL • Current Rheumatology issues (15mins) AY • Current Orthopaedic Issues (10mins) ND • Introduction to pathway (5mins) SL • Pairs to consider pathway (10mins) ALL • Questions/ comments to panel (10mins) ALL
Burden of disease • Incidence of one new case per 1,000 population per year suggests: • 140 new cases per year in PCT • 2 new cases per GP per year • Prevalence of 3%suggests: • 4,000 cases in PCT • 60 cases per GP
Health care activity data • 85 episodes of carpal tunnel decompression in 2003 • 75% (64) SACH • 11% (9) QE2 • 5% (4) HHGH • 2% (2) Stoke Mandeville
CARPAL TUNNEL SYNDROME.West Herts Hospitals Trust. SACH 2005. Adam Young1. Background. • Common • Prevalence ~3% • Incidence ~ 52/100,000 person yrs for men • 149/100,000 person yrs for women • Painful and or unpleasant condition. Acute->chronic. • Loss of function e.g. work disability • Diagnosis made clinically in majority • Conservative treatment effective in majority
CTS2. Problems • Diagnostic difficulties – figures for this in primary care not known • Under and or inappropriate treatment in 1ry/2ry care • e.g. results of West Herts primary care audit project showed that ~50% patients with diagnosis of CTS were offered NO treatment while waiting for 2ry care opinion • Waiting lists for diagnosis and treatment in secondary care.
CTS3. Guidelines • Guidelines for diagnosis & management of CTS • 1995 Rheumatology guidance/advice enclosed
CTS4. One stop Clinical assessment/NCS/EMG clinic • Developed at SACH from 1995 in Dept Rheumatology • All GP letters triaged by AY • Standard clinic assessment +/- NCS/EMG • Management initiated & further advice given to GP • 1 Clinic/week at SACH & 0.5 clinic/wk at HHGH • EMG database generated tables which reflect current service figures are enclosed: • Reasons for referral by year i.e. 2000 to 2004 (n & %) • Reasons for referral by source of referral (n & %) relevant to CTS
One stop Clinical assessment/NCS/EMG clinicSACH EMG database tables • These show Rheumatology Dept performs 350-420 studies/year • 75-82% are CTS referrals, of which • 8% from Hand Surgeons • 22% from orthopaedics • 67% from one stop NCS/EMG clinic