Download
1 / 53
1.62k likes | 5.83k Vues
Carpal Tunnel Syndrome. Department of Osteopathic Manipulative Medicine University of North Texas Health Science Center Texas College of Osteopathic Medicine. Case Presentation.

E N D
Carpal Tunnel Syndrome Department of Osteopathic Manipulative Medicine University of North Texas Health Science Center Texas College of Osteopathic Medicine
Case Presentation • A 42-year-old Caucasian female presents to your office complaining of numbness and tingling in her right hand for approximately one year. The sensation is on the palmar surface of the thumb, index, and middle fingers, and ring finger. She states that sometimes it feels like her hand is “asleep,” while other times it feels like “pins and needles.” The symptoms occur at night and the only relief is “flicking” of the wrist.
Case Presentation • Occasionally, the pain is referred to the forearm and shoulder, but only during an acute flare-up. The patient has worked as a secretary at UNTHSC for the past 15 years. • Physical examination: overweight female in NAD. Sensation full & = bilat; DTR’s 2+ & = bilat; slight atrophy and weakness of the thenar muscle and grip strength on the Rt.; decreased ROM of Rt. wrist compared to Lt.; positive Tinel’s and Phalen’s
Differential Diagnosis • Cervical radiculopathy • Cervical disc herniation • Thoracic outlet syndrome • Diabetes mellitus • Fracture/Dislocation • Carpal tunnel syndrome
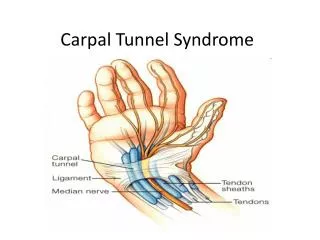
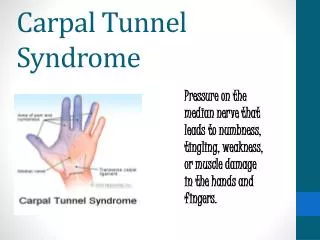
What is Carpal Tunnel Syndrome? • This condition is most commonly described as an entrapment neuropathy of the median nerve at the wrist in the carpal tunnel • The tunnel is formed by the carpal bones and the transverse carpal ligament • Contents of the tunnel include the flexor tendons and the median nerve
ANATOMY • Carpal Tunnel: • space on the volar aspect of the wrist formed by the carpal bones and the transverse carpal ligament (flexor retinaculum).
ANATOMY • Boney Landmarks • Proximal: • pisiform bone - medially • scaphoid bone - laterally • Distal: • hook of the hamate - medial • trapezium bone - laterally
CONTENTS OF CARPAL TUNNEL • I. Median nerve • II. 2 synovial sheathes • 1st sheath • 8 flexor digitorum profundi and superficialis tendons. • 2nd sheath • flexor pollicis longus tendon.
Clinical PresentationCutaneous Innervation • Median nerve cutaneous sensory distribution • Palmar surfaces of • Thumb • Index • Middle • Lateral ½ of ring finger
How does one get carpal tunnel syndrome? • 1. Increase pressure within the canal. • 2. Compromise space within the canal.
Pressure is increased in the carpal tunnel by: • Both flexion and extension of the wrist.
Space is compromised in the carpal tunnel by: • Thickening of the tendon sheaths. • Encroachment from other structures.
Clinical Presentation • Compression of median nerve in carpal tunnel • Anesthesia • Paresthesia • Pain • Muscle weakness • Decreased ROM • Night-time symptoms • “Flick Sign”
Workers involved in specialized tasks: • 1. Require repetitive use of the hand and wrist while held in forced flexion. • 2. Carpal tunnel becomes tighter when wrist held in forced flexion.
Physical Examination • 1. Tinel’s sign • a. lightly tapping over volar aspect of wrist • b. + sign- tingling distally of 1st 3 1/2 digits. • 2. Phalen’s sign • A. George Phalen - hand surgeon of Cleveland clinic. • B.Hyperflex both wrists against dorsal surface of each hand. • C. + test- numbness in approx. 30 sec.
Special TestsPhalen’s & Tinel’s Tests • Phalen’s • Wrist flexion to maximum for 60 sec • Tinel’s • Tapping over transverse carpal ligament • Symptoms • Pain • Anesthesia • Paresthesia
OMT TREATMENT • Transverse Carpal Ligament • Carpal Bones • Interosseous Membrane
Osteopathic Treatment • Myofascial release • Articulatory • Muscle energy
OMT Techniques • Opponen’s Roll • Squeeze with Rapid Circumduction • Wrist & Interosseous Membrane Ligament
Myofascial Release • 1. Pressure applied centrally from the dorsal surface of the carpal bones. • 2. Simultaneously apply pressure to the edges of the carpal bones on the ventral surface of the wrist. (lateral and medial borders of the carpal tunnel.) • 3. Simultaneously the D.O. catches the patient’s thumb and pulls it back into hyperextension with abduction treating the attachment of the abductor pollicis brevis muscle. • 4. Digits and wrist are hyperextended (pulls flexor tendons into canal and distends canal from inside out.)
Opponens Roll Technique • Lateral axial rotation stretches the opponens pollicis muscle. • Thenar abduction with extension and lateral rotation.
Opponen’s Roll • Grasp first digit (thenar emin.) and fifth digit (hypothenar emin.) with each hand • Contact pisiform and scaphoid bones with thumbs • Extend wrist, abduct and laterally rotate first digit with counterforce over hypothenar area • Use thumbs to stretch at boney contact points the transverse carpal ligament in lateral/medial direction • Provide stretch to transverse carpal ligament for 3-5 minutes • Perform at each clinic visit and teach patient to perform technique at home on daily basis
Myofascial Release • 1. Crisscross thumbs over medial and lateral borders of carpal tunnel. • 2. Apply gentle traction. • 3. Have patient abduct fingers and hold in abduction. • 4. With abduction maintained, have patient slowly flex involved wrist over D.O.’s crisscrossed thumbs.
Articulatory Technique • 1. D.O. applies a squeeze between his/her hands, producing traction at the joint as the thenar and hypothenar eminences separate. • 2. D.O. maintains the squeeze and applies the articulatory force as a circumduction of the patient’s wrist in a clockwise, then counterclockwise conical motion, carrying the dysfunction through the restrictive barrier.
Squeeze with Rapid Circumduction • Place heel of both hands over radiocarpal region of carpal bones & interlace fingers • Attempt to distract fingers while squeezing fingers together • Causes the heel of each hand to squeeze together • Circumduct wrist in circular or figure eight fashion • Care should be taken to maintain capsular tension throughout the articulatory sweep • Perform at each clinic visit
Muscle Energy (interosseous membrane) • 1. D.O. thumbs are crossed over the anterior surface of the patient’s forearm with interosseous dysfunction between his/her thumbs. • 2. The pad and tip of the thumb of the hand closest to the D.O. contacts the lateral side of the ulna. The thumb of the other hand contacts the medial side of the radius. • 3. Have patient attempt to pronate palm and use isometric counterforce.
Flexion with Posterior Carpal Glide • 1. Flex wrist to balanced ligamentous tension. • 2. Apply traction. • 3. Move joint into extension to articulate through the restrictive barrier.
Extension With Anterior Carpal Glide • 1. Extend wrist to the point of balanced ligamentous tension. • 2. Apply traction. • 3. Move joint into flexion to articulate the joint through the restrictive barrier.
Abduction with Medial carpal Glide • 1. Wrist in abduction to balance ligamentous tension. • 2. Apply traction. • 3. Move the joint into adduction to articulate the joint through restrictive barrier.
Adduction with Lateral Carpal Glide • 1. Place wrist in adduction to the point of balanced ligamentous tension. • 2. Apply traction. • 3. Move the joint into abduction to articulate the joint through the restrictive barrier.