Carpal Tunnel Syndrome
190 likes | 569 Vues
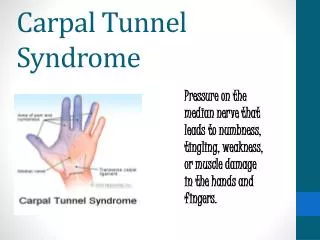
Carpal Tunnel Syndrome. A clinical audit of the local service. Dr Elena Nikiphorou Dr Adam Young Suzanne Jenkins (Research Assistant). Background. Incidence : 1 per 1000 people/year Prevalence : 3% population Gender/age : commoner in F 4:1, peak 45-54 in F, increases with age in M

Carpal Tunnel Syndrome
E N D
Presentation Transcript
Carpal Tunnel Syndrome A clinical audit of the local service Dr Elena Nikiphorou Dr Adam Young Suzanne Jenkins (Research Assistant)
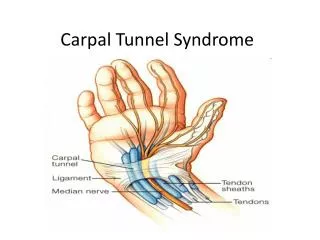
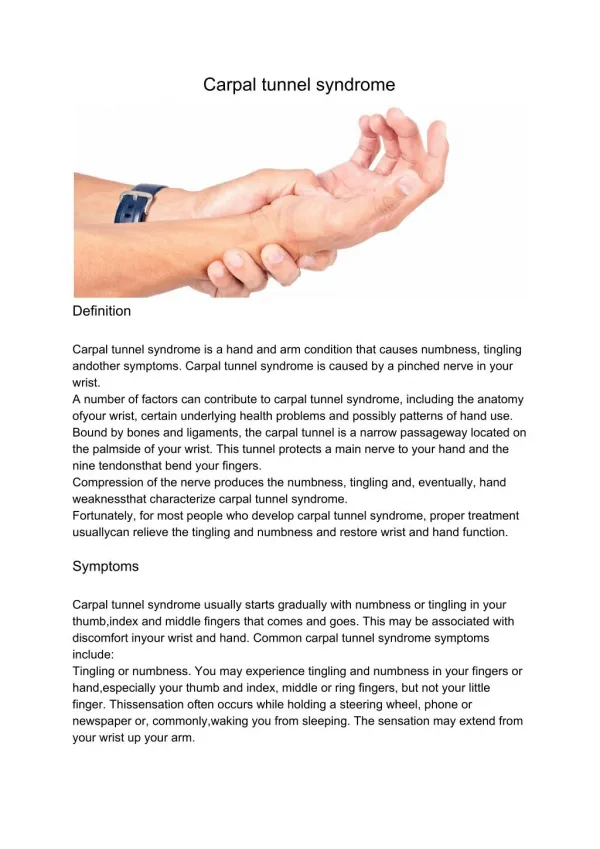
Background • Incidence: 1 per 1000 people/year • Prevalence: 3% population • Gender/age: commoner in F 4:1, peak 45-54 in F, increases with age in M • Pathogenesis: compression of median nerve within the carpal tunnel
Management Clinical CTS Severe symptoms/atypical presentation/uncertain diagnosis Mild symptoms, no clinical signs Moderate symptoms & sensory signs • Simple analgesics • NSAIDs • Wrist splints • OT • Weight reduction Cortisone injection EMG/NCS Day case decompression surgery Care pathway adapted from Laitner & Young (2004)
Why audit? • Management varies between different hospitals • Delays between symptom onset and treatment • 1995 audit with St Albans GPs (51% did not receive any treatment while waiting for 1st hospital referral) • WHHT 2009/10: • 18 week pathway from GP referral to treatment • Are we achieving this target? • Does the one-stop clinic solve the problem?
Referral times 1985-1995 12wks 32wks 4wks 10wks 12wks 24wks T=94wks Neuro OPD Rheuma OPD Ortho OPD Neuro OPD GP NCS/EMG Surgery 10wks 12wks 14 wks 26wks T=62wks Rheuma OPD Ortho OPD GP NCS/EMG Surgery 1995 10wks 20wks T=30wks Rheuma OPD + NCS/EMG Surgery GP One stop One stop Jayakumar K. BJR 2006;45(S1):262
One-Stop CTS clinic • Introduced at SACH & HHGH in 1995 • Clinical assessment (15-30 minutes) • EMG/NCS (15-30 minutes) • Diagnosis? CTS or not ? Radicular origin e.g. C5/6/7 ? Both (“double crush”) ? neuropathy, MND • Further investigations e.g. x-rays C-spine, wrist ultrasound • Assessment of need for surgery or other treatments
Audit • Source and type of referrals • Times from referral to EMG/NCS to surgery • Patient satisfaction • Questionnaires sent to 235 patients, seen between 2006-2010
Graph 1: Yearly Total CTS procedures Days Year
Graph 3: Times to EMG/NCS clinic 360 GP referrals per year Days Year
Patient satisfaction questionnaire (PSQ) • Symptom duration prior to EMG/NCS • Symptom severity pre-treatment • Symptom severity post-surgery • Investigations & Treatment • Overall satisfaction
A unique service Cost effective – reduced number of outpatient clinics (6 to 2!) Waiting times improved Improved patient convenience Improved overall patient satisfaction Conclusions