Download
1 / 32
320 likes | 545 Vues
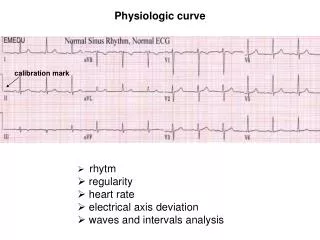
PHYSIOLOGIC MONITORING. Hemodynamic Monitoring - provides information as to the C-P status of the patient - traditional clinical assessment are usually unreliable - major changes in the cardiovascular status may not be clinically obvious - invasive techniques must be utilized.

E N D
Hemodynamic Monitoring - provides information as to the C-P status of the patient - traditional clinical assessment are usually unreliable - major changes in the cardiovascular status may not be clinically obvious - invasive techniques must be utilized
A. Arterial Catheterization 1. Indications a. Need for continuous blood pressure monitoring. b. Need for frequent arterial blood sampling.
Conditions that need continuous and accurate BP monitoring: i. shock states ii. hypertensive crisis iii. surgery in high risk patients iv. use of potent vasoactive or inotropic drugs v. controlled hypotensive anesthesia vi. situations that may lead to rapid changes in cardiac function
2. Contraindications - no ABSOLUTE contraindication to arterial catheterization - RELATIVE contraindications are: a. bleeding problems (hemophelia) b. anticoagulant therapy c. presence of a vascular prosthesis d. local infection
3. Sites of Catheterization a. radial artrery - dual blood supply - most commonly used site - simple canulation - low complication rate - modified “Allen’s” test – assess ulnar artery - Doppler technique, plethysmography, pulse oximetry
b. axillary artery - for long term monitoring - large size - close proximity to the aorta - deep location - technical difficulty in insertion - located near neurovascular structures
c. femoral artery - large size and superficial location - prone to atherosclerosis - difficult to keep clean d. dorsalis pedis e. superficial temporal artery - surgical exposure is required - neurologic complications observed
f. brachial artery - for short term use only - median nerve contracture (Volkman’s contracture)
*Complications of arterial catheterization 1. failure to cannulate 2. hematoma 3. disconnection from monitoring system 4. infection - catheters in place for more than 4 days - surgical insertion - local inflammation 5. retrograde cerebral embolization 6. A-V fistula / pseudoaneurysm 7. severe pain, distal necrosis
B. Central Venous Catheterization 1. Indications a. access for fluid therapy b. access for drug infusion c. parenteral nutrition d. CVP monitoring e. other indications - aspirate air embolism - placement of cardiac pacemaker / vena cava filters - hemodialysis access
*Central Venous Pressure Monitoring 1. useful in hypotensive patients 2. tracings for arrythmias 3. gives information about the relationship between intravascular volume and right ventricular function 4. use of a water manometer for pressure measurements 5. Normal CVP measurement – 5-10 mmH2O
2. Sites of catheterization a. subclavian vein - easiest to cannulate - pneumothorax most common complication - difficult to control bleeding b. internal jugular vein - lower risk of pneumothorax - arterial puncture most common complication c. external jugular vein d. basilic vein
*Complications 1. catheter malposition 2. dysrythmmias 3. embolization 4. vascular injury 5. cardiac, pleural, mediastinal, neurologic injury
II. Respiratory Monitoring - monitoring ventilation and gas exchange * Indications 1. Decision making for the need of mechanical ventilation. 2. Assessment of response to therapy. 3. Optimize ventilatory management. 4. Decision to wean from ventilator.
A. Ventilation monitoring 1. Tidal volume – volume of air moved in or out of the lung an a single breath 2. Vital capacity – maximal volume at expiration after a maximal inspiration 3. Minute volume – total volume of air leaving the lung each minute 4. Phsiologic dead space – the portion of tidal volume that does not participate in in gas exchange a. anatomic dead space b. phsiologic dead space
B. Gas Monitoring - reported as directly measured partial pressures (PO2 and PCO2) - use of pulse oximeters for continuous measurements 1. Blood gas analysis – information about: a. efficacy of gas exchange b. adequacy of alveolar ventilation c. acid – base status
2. Capnography - graphic display of CO2 concentration in wave form - available systems a. infrared analysis b. mass spectrometry c. Raman scattering d. disposable colorimetric devices e. semi-quantitive measurement on the end- tidal CO2 concentration
3. Pulse oximetry - reliable, real time estimation of the arterial Hgb saturation - wide clinical acceptance
4. Gastric Tonometry - relatvely non-invasive monitor of adequacy of aerobic metabolism in organs whose superficial mucosal lining is extremely vulnerable to low flow changes and hypoxemia
III. Renal Monitoring - the kidney is an excellent monitor of adequacy of perfusion - prevention of renal failure - predict drug clearance and proper dose adjustment
A. Urine Output - commonly monitored but may be misleading - normal urine output 0.5 ml/kg/hour - correlates with glomerular filtration rate (GFR) - high output may not accurately reflect GFR ex. Diabetes Insipidus - may be affected by other factors
B. Glomerular Function Tests 1. Blood Urea Nitrogen (BUN) a. affected by GFR and urea production b. increased in TPN, GI bleeding, trauma, sepsis, steroid use c. lowered in starvation, liver disease d. not a reliable test
2. Plasma Creatinine a. more accurate than BUN b. directly proportional to creatinine production c. inversely related to GFR d. not affected by protein or nitrogen production or rate of fluid flow through tubules e. related to muscle mass
3. Creatinine Clearance a. used if values of plasma creatinine are affected by muscle disease b. serial determination of urine is done and is currently the most reliable method of assessing GFR
C. Tubular Function Tests 1. The most reliable test to distinguish pre- renal azotemia from tubular necrosis 2. Requires simultaneous collected urine and blood samples
IV. Neurologic Monitoring - early recognition of cerebral dysfunction - facilitate prompt intervention and treatment A. Intracranial Pressure Monitoring 1. Cerebral Perfusion Pressure - >70mmHg 2. Glasgow Coma Scale
B. Electrophysiologic Monitoring - reflects spontaneous and on-going electrical activity in the brain C. Transcranial Ultrasound - monitors cerebral blood flow - detects vasospasm D. Jugular Venous Oximetry - measures relationship of blood flow to O2 consumption
V. Metabolic Monitoring A. Caloric Demands B. Respiratory Quotient of Food VI. Temperature Monitoring A. Rectal B. Middle Ear C. Esophageal