Download
1 / 24
290 likes | 613 Vues
ImmunoPathogenesis of HIV Disease. Overview of HIV Epidemic Basic biology of HIV-1 Stages of HIV Disease Viral and Cellular Dynamics after HAART HIV Therapy and Future Directions in Pathogenesis Research . Overview of HIV Epidemic. Origin of virus Scope of worldwide Epidemic

E N D
ImmunoPathogenesis of HIV Disease • Overview of HIV Epidemic • Basic biology of HIV-1 • Stages of HIV Disease • Viral and Cellular Dynamics after HAART • HIV Therapy and Future Directions in Pathogenesis Research
Overview of HIV Epidemic • Origin of virus • Scope of worldwide Epidemic • Brief History of Epidemic • Immunodeficiency syndrome identified (GRID) in late 1970’s • Identification of virus and development of serological test - 1984 • Introduction of first antiretroviral drug (AZT) – 1987 • Identification of three stages of disease – early 1990’s • Competitive RT-PCR to measure viral RNA in plasma – 1993 • combination antiretroviral drugs (protease inhibitors & RTI) – 1995 • Introduction of ART to Africa – 2001 • Epidemic still expanding – 2006
Death rates in persons aged 25-44 years in the United States
A global view of HIV infection 38.6 million people [33.4‒46.0 million] living with HIV, 2005
Life cycle of HIV • Viral Entry - CD4 and co-receptors • Reverse Transcription • Integration into host chromatin • Transcriptional activation of integrated provirus • Production of viral proteins, particle assembly and maturation
Chemokine Co-receptors for HIV • Two co-receptors - CXCR4 and CCR5 with distinct viral isolates • CXCR4 - T tropic - syncytium inducing - present in late stage disease • CCR5 - M tropic - non- syncytium inducing - dominant in early infection • Natural ligands - SDF-1/CXCR4 & MIP-1a, MIP-1b, & RANTES/CCR5 • Protection from infection in CCR5 D32 homozygotes
HIV Latent Infection • Pre-integration latency • After reverse transcription, before integration • Due to lability of unintegrated DNA, this pool is dependent on continual de novo infection • Integrated latency • Integrated provirus with low or absent transcription of viral genes (no expression ® no clearance) • Likely the major reason for eradication failure • Controversy about origin, role of defective viral genomes, chromatin integration sites, and clearance rate
High viral mutation rate • Reverse Transcriptase is fairly sloppy and cellular RNA polymerases are not high fidelity enzymes • Estimated to be around 1000 different sequence variants in a single individual at one time • Rapid evolution of drug resistance, if there is continued de novo infection • In general, inverse relationship of “viral fitness” in vivo growth rate and drug resistant phenotype. Wild type virus grows out when drugs withdrawn. • Partial drug mediated inhibition of growth is recipe for resistance
Diagnosis of HIV Infection • Signs & Symptoms of Primary Infection • HIV Ab measurement (EIA Western Blot) • HIV viral RNA in plasma • Response to suspected exposure (needle stick) • Post-exposure prophylactic ART
Laboratory Testing for AIDS • Antibody testing —to diagnose HIV infection. • p24 protein testing —may be used to detect early HIV infection, to monitor HIV therapy and HIV progression, and to screen blood for HIV. • Viral load testing —to decide when to start therapy and to monitor therapy and HIV progression. • In chronic phase, the extent of viremia (as measured by HIV-1 RNA) can predict disease progression • CD4 testing —to decide when to start therapy and to monitor therapy, HIV progression, and the status of the immune system. • >500 asymptomatic • 200-499 early symptoms • <200 severe immunosuppression • Genotypic resistance testing —to determine if a particular strain of HIV is resistant to the therapy you are on and if the therapy should be switched.
Occupational Exposure to HIV • Concept of Universal precautions • Any human bodily fluids could be contaminated with infectious agents transmitted by parenteral exposure. • In case of possible exposure, immedately report to HIV response team (at UAB 4-3675) or ER. • Early Treatment with antiretroviral drugs have very substantial benefit • Time after infection is critical. • Excellent results if ART started within several days.
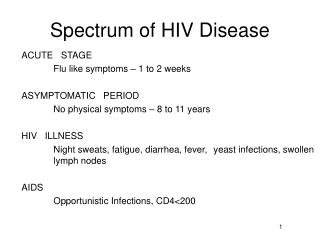
Three Phases of HIV Disease • Acute Infection Syndrome • “flu-like” clinical illness • high viral load that resolves coincident with development of effective CD8 T cell response • Clinical “Latent” Disease • Widely variable viral load correlated with rate of disease progression (loss of CD4 T cells) • Lymphadenopathy and constitutional symptoms • End Stage Disease (AIDS) • CD4 T cells < 200; often increase in viral load • development of opportunistic infections
Viral Dynamics after HAART HAART Initial Rate Independent of Absolute vRNA t½ 1 day
Dynamics of HAART Induction • Rapid fall in viral RNA in plasma • First phase is very rapid (t½ = 1-1.5 days)and fairly consistent among individuals, second phase slower. • Rapid Increase in CD4 T cells in Blood • Redistribution of lymphocytes from inflammed tissue is primary mechanism - previously thought to be change in CD4 T cell growth • Significant Immune Reconstitution • Decreased incidence of OIs and death
Status of HIV Dynamics on HAART • Despite initial optimism, infection not eradicated • Concept of Reservoir- residual viable virus during HAART • Latently infected CD4 T cells • Sequestered Anatomic site - CNS, ?others • Persistent rounds of de novo infection • Intermittent Non-adherence • Slow evolution of viral quasispecies sequences • Both Latent infection and persistent vRNA+ cells - Tissue and Blood
Goals in Medical Management of HIV Disease • Pharmacological suppression of viral Replication • Multiple drugs available – low replication low mutations • Monitoring status – viral load and CD4 count • Eradication - complete elimination of viable virus • Problems - HAART alone does not result in Eradication. • Regimen is difficult - Intermittent regimen Non-Adherence • Development of Drug Resistance • Persistent population of latently infected CD4 T cells • Induction of Immune Control • Increase efficiency of immune response to viral antigen to maintain control of replication at very low viral load • Low viral load = Lack of disease progression • Normal “successful” outcome of chronic viral infection