Download
1 / 64
640 likes | 655 Vues
Malnutrition and obesity. CONF.DR.INGRITH MIRON DR. MOCANU ADRIANA. What is malnutrition?. World Health Organization definition:

E N D
Malnutrition and obesity CONF.DR.INGRITH MIRON DR. MOCANU ADRIANA
What is malnutrition? World Health Organization definition: The term is used to refer to a number of diseases, each with a specific cause related to one or more nutrients (for example, protein, iodine or iron) and each characterized by cellular imbalance between the supply of nutrients and energy on the one hand, and the body's demand for them to ensure growth, maintenance, and specific functions, on the other.
HUMAN NUTRITION • Obesity & under-nutrition are the 2 ends of the spectrum of malnutrition. • A healthy diet provides a balanced nutrients that satisfy the metabolic needs of the body without excess or shortage. • Dietary requirements of children vary according to age, sex & development.
Macro andmicro nutrients • Macro-nutrients • Protein (amino acids) • Energy (carbohydrates) • Fat (fatty acids) • Micro-nutrients • Water soluble vitamins (assist in energy-release of carbohydrates and red blood cell formation) • Fat soluble vitamins (development & metabolism) • Minerals
Malnutrition: definition • Malnutrition : chronic state of nutrition due to insufficient food intake (caloric and / or protein) specific for infants and small child. • Along with major deficits of nutrients occur also deficiencies in vitamins and minerals (deficiency anemia, rickets, avitaminoses). • Depression of cellular immunity caused by malnutrition favors increased susceptibility to infection, which worsens the initial deficit, the infection is often the one that causes death. • Half of the states of malnutrition : first 6 months of life, overlapping maximum period of CNS development (neuronal proliferation - to a maximum of 18 months).
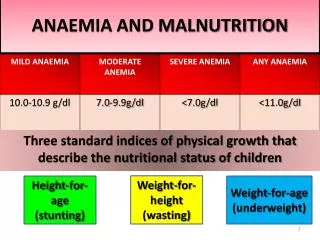
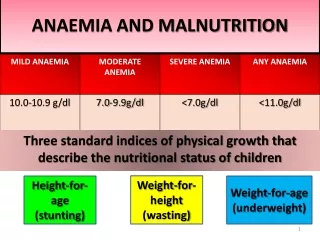
Types of malnutrition • Severe Protein-Energy Malnutrition (>3 S.D.) • Kwashiorkor (low protein) • Marasmus (low calories) • Mild/moderate undernutrition (>2 S.D.) • Stunting • Underweight • Wasting • Micro-nutrient deficiency • Iodine • Iron • Vitamin A • Vitamin D
OVERVIEW OF MALNUTRITION • The majority of world’s children live in developing countries • Lack of food & clean water, poor sanitation, infection & social unrest lead to LBW & PEM • Malnutrition is implicated in >50% of deaths of children <5years (5 million/yr).
OVERVIEW OF MALNUTRITION • WHO estimated that 32% of children in developing countries are underweight (182 million). • 78% of these children live in South-east Asia & 15% in Sub-Saharian Africa. • The reciprocal interaction between PEM & infection is the major cause of death & morbidity in young children.
EPIDEMIOLOGY • The term protein energy malnutrition has been adopted by WHO in 1976. • Highly prevalent in developing countries among children <5 years; severe forms 1-10% & underweight 20-40%. • All children with PEM have micronutrient deficiency.
Classification/Terminololgy The term malnutrition (Anglo-Saxon School) or dystrophy (French School) define the states of malnutrition through food intake deficiency- qualitatively and/or quantitatively. • Protein energy malnutrition (PEM); • Protein malnutrition (PM).
Classification/Terminololgy WHO proposes 2terms (referring to states of severe malnutrition) • Marasmus - severe PEM; • Kwashiorkor - severe PM. These terms are unsatisfactory for practice - do not include light and intermediate states of malnutrition→new terminology. WHO - classification of malnutrition • Primary malnutrition • Secondary malnutrition.
Primary Malnutrition :ETIOLOGY Primary malnutrition • correctfood intake; • negativ prognosis due to disturbed growth that can not be influenced therapeutically (frequent association with mental deficiency); • commonly associated with: fetal malnutrition, low birth weight and small height sometimes. The causes of primary malnutrition: • organics (severe malformations: renal, digestive, cardiac) • genetically conditioned diseases (chromosomal, metabolic) • fetal infections (toxoplasmosis, syphilis, cytomegalovirus).
Etiology of Primary Malnutrition • Failure of lactation. • Improper weaning practices • Poverty • Food taboos • 2 or more children under 5 years of age in same household • Death of mother • Incompetent/ ignorant mother. • Lack of family planning
SECONDARY MALNUTRITION Secondary malnutrition (exogenous): • deficiency due to dietary intake qualitatively or quantitatively, • prognosis is generally good by correcting the cause and food intake , • usually no mental deficits.
SECONDARY MALNUTRITION Classification of secondary malnutrition (WHO): I. Moderate malnutrition: - mild (grade I dystrophy, hypotrophy, "poor child"); - medium (grade II dystrophy); II. Severe malnutrition (grade III dystrophy): - energy-protein malnutrition (PEM) :marasmus, atrepsia; - protein malnutrition (PM) • acute form (kwashiorkor); • chronic form (marasmickwashiorkor ).
Etiology of secondary malnutrition A)Dietary deficiency • quantitatively: native hipogalactia; late diversification over 6 months of age; improper dilution of milk, restrictive diets, taboos related to food, family, religious, ethnic; • quality: carbohydrate deficiency ( cow’s milk distrofy ), protein deficiency (edematous dystrophy by excess flour, using vegetable protein low biological value), lipid deficiency ( regimes without lipids) • lead to imbalance by decreasing caloric intake.
Etiology of secondary malnutrition B) infections:entericinfection;bronchopneumonia, otomastoidite, chronic urinary tract infection, bacterial or parasitic diarrhea, syphilis, tuberculosis- poor appetite, digestive losses, increased catabolism. c) psychosocial events:maternal deprivation, neglect of physiological rhythm of alimentation, lack of hygiene, pollution, cold, hospitalism;
Etiology of secondary malnutrition D) psychosomatic disorders : - anorexia , • organic disease (hypertrophic pyloric stenosis, congenital malformations that cause repeated vomiting, cystic fibrosis, celiac disease, congenital intolerance to disaccharides, labio-maxillo-palatine cleft) , • infantile cerebral palsy with impaired swallowing, pharyngeal incoordination.
Etiology of secondary malnutrition Chronicillnessesthatcommonly are associatedwithnutritionaldeficiencies include thefollowing: • Cysticfibrosis • Chronic renal failure • Childhoodmalignancies • Congenital heartdisease • Neuromuscular diseases • Chronicinflammatoryboweldiseases
Etiology of secondary malnutrition • In addition, thefollowingconditions place children at significantrisk for thedevelopment of nutritionaldeficiencies: • Prematurity • Developmentaldelay • In uterotoxinexposure (ie, fetal alcoholexposure) • Childrenwith multiple foodallergiespresent a special nutritionalchallengebecause of severe dietaryrestrictions. Patientswith active allergicsymptomsmayhaveincreasedcaloricandproteinneeds.
Protein-energy malnutrition pathogenesis In severe forms when nutritional deficit exceeds a certain limit, the consequences are severe: • regression of all metabolic activities (decreased basal metabolism, decreased intracellular water, decreasing opportunities to retain water and salt); • low digestive tolerance (decreased activity of disaccharideses, pancreatic secretion, bile acids); • loss of defense to infection. Very low digestive tolerance and dietary intake can not maintenance energy needs lead to autophagic processes (the metabolism of starvation).
Protein-energy malnutrition pathogenesis Severe lack of calorie and protein → hypoglycemia, decreased serum amino acids in pancreatic reaction → → hipoinsulinism (main endocrine changes in starvation) → decrease peripheral insulin and the appearance adaptive responses: • mobilization of fatty acids from adipose tissue (lipolysis) to the liver to be an energy source; • decrease in muscle glucose utilization and incorporation of amino acids that are directed to the liver, where they are used for protein synthesis and neoglucogeneză (the exhausted body fat); • hepatic protein synthesis is achieved by sacrificing muscle proteins.
Protein-energy malnutrition pathogenesis Infection - is the vicious circle in severe malnutrition, worsening starvation and being the main cause of death by: • loss of appetite; • digestive losses (diarrhea); • increased catabolism (febrile illness); • disorders of intermediary metabolism by reducing metabolic efficiency of nutrients; • increased urinary nitrogen loss, K, Mg, Zn, P, vitamin A, C, B2.
Pathogenesis of protein malnutrition The acute form (typical Kwashiorkor) • occurs after 6-8 months; • diversification normal calorie but devoid of protein; • deposits of fat are consumed, stature is normal and causes severe loss of protein (proteins from the liver, muscle, pancreatic proteins, serum albumins deficiency) and loss of intracellular K (preservation mitosis), hepatic fatty infiltration if infection occurs - marked reduction albumin (hepatic synthesis deficient) → fluid retention (decrease in colloid osmotic pressure capillary) → edema.
Pathogenesis of protein malnutrition Chronic form (MarasmicKwashiorkor) - secondary selective protein intake deficiency is characterized by: - sufficient caloric intake; - normal secretion of insulin: • favors lipogenesis (fatty acids are not available in place of amino acid oxidation - fatty tissue is preserved); • reduced level of plasma amino acids by three mechanisms: • reduce the release of amino acids from muscle; • stimulates the passage of serum amino acids in muscle; • favors the the incorporation of amino acids into the muscle.
MARASMUS/KWASHIORKOR • Marasmus represents an adaptive response to starvation, whereas kwashiorkor represents a maladaptive response to starvation • In Marasmus the body utilizes all fat stores before using muscles.
Assessment of NutritionStatus • Clinical • Anthropometric • Dietary • Laboratory
Investigations for PEM • Full blood counts, inflammatory markers; • Blood glucose profile, lipidic profile • Iron, vitamin levels; • Microbiology: septic screening,stool & urine for parasites & germs; • Electrolytes, Ca, Ph & Mg; • Serum proteins, protein electrophoresis; • immunological status: cellular immunity - decreased T cell, interferon, IDR lack of response to tuberculin; humoral immunity - low IgA (secretoryIgA), IgM - high, low IgG. • Decrease complement C3; • Exclude HIV & malabsorption.
Investigations for PEM In essence: • decrease serum albumins → edema; • decrease apoproteins (lipoproteins carrier); • storage of fat in the liver (fatty infiltration); Clinical outcomes: oedema, hepatomegaly (fatty liver), changes in hair growth and skin (areas of hypo-or hyperpigmentation, fissures), diarrhea (villous atrophy), predisposition to infection (humoral and cellular immunity disturbed).
Anthropometric assessment of malnutrition anthropometric criteria : • percentiles method (normal 10-90). • standard derivations method (normal + / - 2 SD). • ponderal index (PI) PI = actual weight of the child / ideal weight (W of child of the same age located on the 50th percentile of the growth curve). After the PI values : 3degrees of PEM(Gomez) • degree I (PI = 0.89 to 0.76); • degree II (PI = 0.75 to 0.60); • degree III ( PI = 0.60). PI = 0.90- underweight or child at risk of malnutrition.
Anthropometric assessment of malnutrition The protein malnutrition are two degrees: • degree I PI = 0.8-0.6 - KWASHIORKOR; • degree II PI= 0.6 – MARASMIC KWASHIORKOR Nutritional index (NI) - index diets. • NI= actual weight / weight appropriate waist. After this indicator there are 3 degrees of malnutrition: • grade I (NI= 0.89 to 0.81); • grade II (NI= 0.80 to 0.71); • grade III (NI= 0.70). Head circumference (HC) - highlights the true growth in the first two years. Midarm circumference (measured at the ½ distance between the acromion and olecranon) pathological - under 13 cm - available in children over 2 years.
Assessment of malnutrition- functional criteria Appreciation of the digestive tolerance: • paradoxical reaction to hunger (disproportionate weight loss); • food paradoxical reaction (weight loss to increased food intake, sometimes diarrhea); • sensitivity to fasts - by spacing meals: hypoglycaemia, especially nocturnal → apnea, sudden death. • immunological reactivity : - increased responsiveness to infection; - reactivity collapsed (serious infection without fever, leukocytosis, sometimes opportunistic).
Assessment of malnutrition Neuropsychological development: • Archaic reflexes; • Muscle tone; • Posture; • Mobility; • Development of language; • Affection. They are affected differently depending on the severity of malnutrition .
Clinical features in marasmus • Marked muscle wasting and loss of subcutaneous fat; • Monkey facies; • Skin becomes loose and hangs in folds; • Abdomen protuberant due to hypotonic muscles; • Temperature is usually sub-normal; • Child is alert.
Clinical features of kwashiorkor • Generalized edema more marked in lower extremeties, muscle wasting; • Growth retardation; • Psychomotor changes; • Apathy and irritability; • Fine and discolouredhair; • Anemia; • Usually flaky paint dermatitis; • Enlarged liver due to fatty changes.
Complications of PEM • Hypoglycemia • Hypothermia • Hypokalemia • Hyponatremia • Heart failure • Dehydration & shock • Infections (bacterial, viral & thrush)
TREATMENT: Prevention of Malnutrition • Primary Prevention • Health Education to mothers about good nutrition and food hygiene • Immunization of children. • Growth monitoring on Growth Charts specially of all children under 3 years of age • Secondary Prevention • Mass Screening of high risk populations, using simple tools like Weight for age . • Tertiary Prevention • Good Nutritional Care, supplementary feedings and rehabilitation, counselling of mothers.
TREATMENT: Prevention of Malnutrition • Natural nutrition - first 4-6 months; • Artificial nutrition - milk type, dilution, enrichment rice mucilage; - Compliance with immunization schedule, the correct treatment of infections; - Inadequate conditions and social environment.
TREATMENT OBJECTIVES: • accurate assessment of the form and degree of malnutrition; • pointing out the main deficiencies (protein, fat, carbohydrates, fluid and electrolyte minerals and vitamins), immune status and the possibility of co-infection; • finding the cause which produced malnutrition; • recovery plan individualized for the nutritional deficiency as quickly as possible.
TREATMENT General principles: The recovery of PEM (II and III degree) : I. The initial phase •Correction of water & electrolyte imbalance; • Treatment of infectious complications. II. Repair phase • Dietary therapy; • Correction of deficiencies (anemia, rickets, hypovitaminosis, etc). III. Convalescence phase • Restoration of body composition; • Enhancing healing. Optimal objective is to resume growth after 2-3 weeks of starting the diet and clinical recovery in 6-8 weeks.
TREATMENT I)Parenteralnutrition for 2-3 days →enteral nutrition with flow probe using hyperproteic and hypercaloric solutions ; II) Early initiation of oral nutrition : hypoallergenic preparations rich in proteins and calories, low osmolarity:Alfare, PeptiJunior, Pregestimil, Nutramigen, Pregomin or amino acid formulas, such as Neocate . • Keep in parallel parenteral intake of carbohydrates, amino acids, lipids. • Simultaneously treating infections, hypoproteinemia, anemia, multivitamins deficiencies . • This variant is also little used because it requires specials dietetics and carefully monitorization of nutritional therapy .
TREATMENT III) after fluid replacement and electrolyte - digestive tolerance : • with carrot soup or rice mucilage (in various concentrations ) in a dose of 150-200 ml / kg ( not exceeding 1000 ml / day) • carbohydrates were obtained from glucose 5%, 7 %, 10 % and chicken mixed proteins ( hypoallergenic, 100g , 17g protein). • after normalization of the stools ( 7 days) :oil gradually (3-4 ml / day ) and after 10 days from the beginning of enteral diet →hypoallergenic preparation can be inserted (!preparations lactose free- can induce cow's milk protein intolerance ) . • week 4 :sugar (restoring lactose tolerance is difficult , 3-4 months); • flour products containing gluten will not enter until full recovery; • increases in protein - calorie intake by parenteral administration of carbohydrates , amino acids and proteins; • treat the infection , iron or vitamin deficiencies .
TREATMENT Malnutrition has its weight age. • correct food intake : 8-10% protein, 54-50% fat, 50-60% carbohydrates: 1 g lipid- 9 kcal; 1 g protein - 4.1 kcal; 1 g carbohydrate - 4.1 kcal. • complete metabolism of 1 g of protein are required 35-40 kcal. • a protein intake ˃5 g / kg / day is dangerous, resulting hyperammonemia, increased blood urea nitrogen ; • Increasing K intake to 4-5 mEq / l .
TREATMENT Recovery of PEM degree II(advenced) and III (Suskie) contains: • calorie - 175 kcal / kg / day; • protein - 4 g / kg / day; • lipid - 9.59 g / kg / day; • carbohydrate - 18.3 g / kg / day. • Research and treating infection with antibiotics (ideally etiologic) is mandatory. • In severe malnutrition ↓ IgG: iv administration of gamma globulin • protein malnutrition (low albuminandproteinemia ): human albumin administered iv (1 g / kg / day). • basal energy needs - 70 kcal / kg / day.
TREATMENT Mild forms of MPC • Treat at home by correcting the diet (food ration for age - increasing protein intake to 0.5-1 g / kg / day→ 20 to 30 kcal / kg / day). • correction of the causes: maternal hipogalactia,hypocaloriec diet with incorrect mixed or artificial nutrition, extending over six months natural nutrition with delayed/incorrect diversification. • Quick recovery in 1-2 weeks.
TREATMENT PEM (severe forms degree II-III , III) • Treat only in hospital. • The first 24 hours - fluid replacement and electrolyte and acid-base fluid resuscitation. • The following 48-72 hours (sometimes more) partial or total parenteral nutrition, reaching 80-90 kcal / kg / day.
TREATMENT • the rate of protein :4-5 g / kg / day (increasing protein is progressively 1-1.5 g / kg / day, reaching in 4-5 days at this rate) • 180-160 kcal / kg to 180-200 kcal / kg / day • from day 3-4 start exploratory digestive maintaining iv administration sugars, amino acids ; • Diet exploratory :rice mucilage 3%, 5%, 8%; carrot soup 300 ‰ or 500 ‰, • sweetener - glucose 5%, 7%, 10% (even 15%). • 7-8 lunches, from 30-50 ml ground in 2-3 days, if tolerance is good - 140-150 kcal / kg.
TREATMENT Criteria to follow: • normalization of the stools ; • growth rate - slow resume after 2-3 weeks to restore digestive tolerance and achieve optimum value caloric and protein intake (early treatment can decrease the growth rate - restore electrolyte balance, after the disappearance of edema). • avoid prolonged fasts - risk of hypoglycaemia. • immune recovery 25-30 days after initiation of dietary therapy. • histochemical normalization of intestinal mucosa after 3-4 months.
OBESITY Obesity-chronicdisorder of thenutrition in infants, childrenandadolescentscharacterizedbytheaccumulation of fat in adiposetissueandothertissuesandorgans as a result of energyimbalance. The prevalence of thediseaseis on therise: accordingto WHO 22 millionchildrenunder 5 years are obese, theprevalencebecoming triple in thepast 30 yearsandovercomingtheprevalence of malnutrition. For childrenwhohave an overweight or obeseparent, therisk of becomingobeseadultsishigherthan in normal weightchildren. Ifbothparents are obese, a child'srisk of becomingobeseis 80%. 80% of obeseadolescentsbecomeobeseadults.
OBESITY Obesityis a plurifactorial disease, favorablefactorsbeing: • prenatal factors: maternal caloric intake, maternal diabetes, dismaturity, smallsizeandsmallheadcircumference at birth; • perinatalfactors: cold climate at birth. • post-natal factors: theintensity of theincrease in body fatbytheage of 1 year, artificial feedingfrombirth, adolescenceweight.