Download
1 / 51
570 likes | 1.85k Vues
PRINCIPLES OF D ETECTION OF RADIATION INJURES. Accidental dosimetry. BIOLOGICAL DOSIMETRY. PHYSICAL DOSIMETRY. CLINICAL DOSIMETRY. CYTOGENETIC DOSIMETRY Dicentrics, FISH, PCC, MN A . DOSE RECONSTRUCTION , Personal Dosimeters. NAUSEA, V OMITING, BLOOD CELLS COUNTS,

E N D
Accidental dosimetry BIOLOGICAL DOSIMETRY PHYSICAL DOSIMETRY CLINICAL DOSIMETRY CYTOGENETIC DOSIMETRY Dicentrics,FISH, PCC, MNA DOSE RECONSTRUCTION, Personal Dosimeters NAUSEA, VOMITING, BLOOD CELLS COUNTS, SKINREACTIONS... OTHER BIOINDICATORS
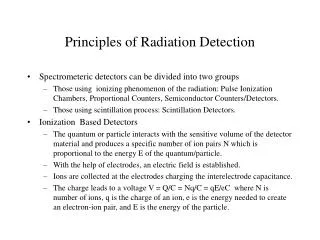
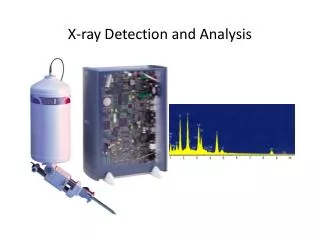
Instruments for detecting and measuring radiation • Survey meters • Geiger-Mueller (GM) instruments • Ionization chamber instruments • Scintilation instruments • Laboratory counters • Personnel dosimeters • Photographic film dosimeters • Thermoluminescent dosimeters • Pocket dosimeters
Level of radioactive contamination Radiation dose rate in area Identity and quantity of radioactive material Accumulated dose to individuals inarea Primary use of radiation instrument Survey meters Laboratory counters Personnel dosimeters
Personnel dosimeters Electronic dosimeter Film badge TLD
Advantages Permanent record Energy and nature of exposure Cost Disadvantages Energy dependence Fading Size Photographic film dosimeters
Clinical and laboratory sings of acute radiation syndrome • Prodromal clinical effects • Time of onset • Degree of symptoms • Haematological changes • Lymphocyte counts • Leukocytes counts • Biological dosimetry
Clinicaldosimetry at radiation vomiting Crude estimate of absorbed dose obtainable from clinical presentation • Vomiting • Onset: 2 h after exposure or later • Onset: 1-2 h after exposure or later • Onset: earlier than 1 h after exposure • Onset: earlier than 30 min after exposure MILD ARS (1-2 Gy) MODERATE ARS (2-4 Gy) SEVERE ARS (4-6 Gy) VERY SEVERE ARS (6-8 Gy)
Radiation dose under 5 Gy • No immediate life-threatening hazard exists • Prodromal symptoms of moderate severity • Onset > 1 hour • Duration < 24 hours
Fatal radiation • Nausea and vomiting within minutes(during the firsthour) • Within hours (on the first day): • Explosive bloody diarrhoea • Hyperthermia • Hypotension • Erythema • Neurological signs
Triage categories of radiation injuries according to early symptoms
No vomiting Vomiting 2-3 h after exposure Vomiting 1-2 h after exposure Vomiting earlier than 1 h, other severe symptoms, like hypotension hyperthermia, diarrhea, oedema, erythema, CNS symptoms < 1 Gy 1-2 Gy 2-4 Gy > 4 Gy Outpatient with 5-week surveillance Surveillance in a general hospital (or outpatient for 3 weeks) followed by hospitalization Hospitalization in a hematological department Hospitalization in a well equipped hematological or surgical department with transfer to a specialized centre for radiopathology Guide for management of radiation injuries on the basis of early symptoms
Clinical signs of skin injury depending on dose of radiation exposure
Laboratorydosimetry using early changes in lymphocyte counts
Degree of ARS Dose (Gy) Lymphocyte counts (cells/L) 2 days after first exposure Preclinical phase Mild Moderate Severe Very severe Lethal 0.1-1.0 1.0-2.0 2.0-4.0 4.0-6.0 6.0-8.0 >8.0 1500-2500 700-1500 500-800 300-500 100-300 0-50 Change of lymphocytes counts depending on dose of acute whole body exposure
Cytogenetic dosimetry Analysis of chromosomal aberrations in peripheral blood lymphocytes - widely used biologicaldosimetry method forassessing radiation dose, especially useful • in persons not wearing dosimeters while exposed to radiation • in cases of claims for compensation for radiation injuries not supported by unequivocal dosimetric evidence • for validation of occupational radioprotection cases involving suspected low-dose exposures
Biophysical background to chromosome damage High LET ***************************** * * * * * * * * Low LET
Classification of chromosomal aberrations Asymmetrical (UNSTABLE) Breaks Symmetrical (STABLE) Centric Ring Inversion Intrachange Interchange Translocation Dicentric
Biological dose assessment using standard dicentric analysis • Introduced by M. Bender in 1964 • Isolated lymphocytes stimulated by phytohaemagglutin (PHA) into mitosis • Arrest of metaphase using colchicine • Scoring of dicentric chromosome aberrations in metaphase spreads
Dicentric chromosome aberrations in metaphase spreads dic f dic f f f
Dose curves at high LET and lowLET radiation Y = A+aD + bD2
Dose curvesatacute andchronic exposure particles Fast neutrons (High LET) Gamma rays, X-rays acute exposure (Low LET) Y = c + aD Y = c + aD + bD2 Effect Dicentric yield Y = c + aD Gamma rays X-rays chronic exposure (Low LET) Dose
Dose estimationof a partial bodyradiation exposure (non-uniform irradiation)
Dicentric assay • Most accurate method for dose estimation with sensitivity threshold of about 0.1 Gy for whole body low LET radiation • Especially useful • in cases where dosimeter not used, e.g. radiation accident • to support physical dosimetry results in radiation protection and safety practice • to determine partial body exposure not detected by locally placed dosimeter
Limitations of dicentric analysis for dose estimation • Dicentrics are unstable and lymphocytes carryingaberration elimininated with time (average lifetime 150-220 days, depending on dose), hence can underestimate magnitude of dose • Method useful only within few months of irradiation
Translocation assay • Inretrospective dosimetryandchronic exposurereciprocal translocations used for dose assessment • Translocations consideredstablein cell division so yield should not fall with time • Typically detected using specific whole chromosome DNA hybridization probes and FISH methodology
Stable chromosome aberration analysis with G-banding An idiogram showing the banding patterns of individual chromosomes by fluorescent and Giemsa staining A normal G banded male karyotype
Stable chromosome aberration analysis with FISH Translocation Deletion
Applicability of stablechromosome aberration analysis for biological dosimetry • Method based on scoring stable chromosome aberrations (translocations and insertions) detected with fluorescent in-situ hybridization of whole chromosomes • Requires complex procedures and technical equipment • May be use decades after exposure • Sensitivitythreshold a few cGy but method not feasible for doses less than 0.2 Gy because of expense and time needed for analysis • Spontaneous level of stable chromosome aberrations not well established
Premature chromosome condensation (PCC) assay • Initially introduced by Johnson and Rao (1970) • Mitotic-inducer cells (i.e. CHO) isolated using chemical (colcemid) and physical (rapid shaking of flask) technique • Test cells (i.e. human lymphocytes) fused with CHO cells using polyethylene glycol (PEG) • Interphase DNA of test cells condense into chromatid/chromosome-like structures (46 for non-irradiated human cells)
PCC technique CHINESE HAMSTER OVARY (CHO) CELLS (Grown in BrdU) COLCEMID MITOTIC SHAKE OFF (METAPHASE CELLS) FUSE IN PEG PERIPHERAL BLOOD CHO LYMPHOCYTES FICOL SEPARATION Incubate 1 h (Medium+PHA+Colcemid) PCC
PCCs and FISH Irradiated cells with excess break Unirradiated control
Applicability of PCC assayfor biological dosimetry • Dose estimates obtainable within48 hours of receipt of blood inlaboratory • Radiation inducedmitotic delay does not interfere with assaysince performed on interphase nuclei and does not require cell division • Method envisioned applicable afterpartial-body/ supra-lethal exposure and improves detection level oflower doses
Micronucleus assay Cytochalasin B
Micronucleus and nucleoplasmic bridges in binucleated cells B A
Micronucleusassay with pancentromeric probe A B centromere positive centromere negative
Application of micronucleusassay for biological dosimetry • Micronucleus not specific toradiation exposure • Discrimination between total and partial body exposure moredifficult • High doses of radiation interfere with cell division • High baseline frequencyand age dependency make reliability of assay questionable
Glycophorin A (GPA) somatic cell mutation assay • Performed by two-color immunofluorescence flow cytometry on peripheral blood erythrocytes • Based of measuring N/0 variants of erythrocytes, which display phenotype consistent with loss of expression of GPA (M) allele • Can be performed only on individuals heterozygous at this locus that codes for the N/M blood group antigens (approximately half of population) • Prompt but requires complex and expensive equipment • Sensitivity threshold about 0.2-0.25 Gy
Application of GPAassay for biological dosimetry Relationship between glycophorin A mutant frequency in red blood cells and radiation dose for about 1200 A-bomb survivors
Biophysical assays - ESR(electron spin resonance) • Persistent free radicals formed in solid matrix biomaterial (e.g. dental enamel, nailclippings, hair) from accidentally exposed victim can be detected via ESR • Measurements provide reliable biophysical dose estimates and partial body exposure information • In some circumstances, certain clothing material, particularly hard plasticsand buttons, may be measured and absorbed dose estimated
Summary of lecture • In radiation accidents, important to estimate the absorbed doses in victims to plan appropriate medical treatment • In most accidents, physical dosimetry of absorbed dose is not possible. Even where possible, important to confirm the estimates by other methods • Most commonly used method cytogenetic analysis of chromosomal aberration in peripheral blood lymphocytes using dicentrics, translocations, PCC and micronuclei assays