Download
1 / 67
670 likes | 687 Vues
An integrative review of epidemiological data and prevention literature, highlighting the importance of effective alcohol policies in addressing the rising alcohol-related problems and challenges faced by developing nations. This book explores the economic, social, and health impacts of alcohol as a commodity and provides insights into the harmful effects of alcohol consumption.

E N D
Alcohol: No Ordinary CommodityPart I: Establishing the Need for Alcohol Policy Thomas F. Babor, Ph.D., MPH University of Connecticut School of Medicine Farmington, CT USA
Alcohol, No Ordinary Commodity: Research and Public Policy Sponsored by: The World Health Organization and The Society for the Study of Addiction (UK) All royalties from book sales go to the SSA. Authors received no financial support for their work on the book. Authors had no financial conflicts of interest to declare.
The Alcohol Public Policy Group* Co-authorsAcademic Affiliations Thomas Babor University of Connecticut (USA) Raul Caetano University of Texas (USA) Sally Casswell Massey University (New Zealand) Griffith Edwards National Addiction Centre (United Kingdom) Norman Giesbrecht University of Toronto (Canada) Kathryn Graham Centre for Addiction and Mental Health (Canada) Joel Grube University of California (USA) Paul GruenewaldUniversity of California (USA) Linda Hill University of Auckland (New Zealand) Harold Holder University of California (USA) Ross Homel Griffith University (Australia) Esa Österberg Institute for Social Research (Finland) Jürgen Rehm University of Toronto (Canada) Robin Room Stockholm University (Sweden) Ingeborg Rossow National Institute for Alcohol and Drug Research (Norway)
Alcohol, No Ordinary Commodity:Research and Public PolicyOxford University Press (2003) An integrative review of epidemiological data and prevention literature, based on: • International research on alcohol consumption trends and the global burden of disease attributable to alcohol • Growth of the knowledge base on policy-related strategies and interventions • New understandings of the policymaking process at the local, national and international levels
Alcohol policy and alcohol science in developing societies • As economic development occurs, alcohol consumption and resulting problems are likely to rise with rising incomes, confronting developing nations with greater levels of alcohol-related problems, and new challenges to develop effective alcohol policies. • With the growing emphasis on free trade and free markets, international institutions such as the World Trade Organization have pushed to dismantle effective alcohol control measures, including state alcohol monopolies and other restrictions on the supply of alcoholic beverages. • Developing countries badly need their own assessments of their own alcohol policy experiences and their own alcohol science. The world research community in partnership with international agencies has a special responsibility to rectify this situation.
ALCOHOL IS A COMMODITY • Alcoholic beverages are an important, economically embedded commodity • The production and sale of commercial alcoholic beverages generates: • profits for farmers, manufacturers, advertisers, and investors • employment for people in bars and restaurants • tax revenues for the government. • Non-commercial alcohol in developing societies has a traditional role in the local economy
ALCOHOL: NO ORDINARY COMMODITY • The benefits connected with the production, sale, and use of this commodity come at an enormous cost to society. • Three important mechanisms explain alcohol’s ability to cause medical, psychological, and social harm: • physical toxicity • intoxication • dependence
Physical Toxicity • Alcohol is a toxic substance in terms of its direct and indirect effects on a wide range of body organs and systems. Non-commercial alcohol can have additional toxic effects because of additives. • Drinking patterns that promote frequent and heavy alcohol consumption are associated with chronic health problems such as liver cirrhosis, cardiovascular disease, and depression.
Alcohol related chronic disease • Cancer: Mouth & oropharyngeal cancer, Esophageal cancer, Liver cancer, Female breast cancer • Neuropsychiatric diseases: Alcohol use disorders, unipolar major depression, epilepsy • Diabetes • Cardiovascular diseases: Hypertensive diseases, coronary heart disease, stroke • Gastrointestinal diseases: Liver cirrhosis • Conditions arising during perinatal period: Low birth weight, fetal alcohol spectrum disorder
Moderate Drinking: Positive and Negative Effects • Moderate drinking is linked to an increased risk of cancer and other disease conditions. • Regular, light, and moderate alcohol consumption has a cardioprotective effect at the level of the individual drinker. This effect applies mainly to the age group of 40 years and older, where the overwhelming majority of coronary heart disease occurs • But at the population level, there may be no net protective effect from an increase in alcohol consumption, and even a detrimental effect in societies with heavy episodic drinking patterns. • While there may be some offsetting psychological and cardio-protective benefits from drinking, alcohol accounts for a significant disease burden worldwide and is related to many negative social consequences. (Murray & Lopez, 1996; Rehm and Sempos 1995a, 1995b).
INTOXICATION • The main cause of alcohol-related harm in the general population is alcohol intoxication. • Drinking patterns that lead to rapidly elevated blood alcohol levels result in problems associated with acute intoxication, such as accidents, injuries, and violence.
Alcohol related injury • Unintentional injury: • Motor vehicle accidents, • drowning, • falls, • poisonings, • other unintentional injuries • Intentional injury: • Self-inflicted injuries, • homicide, • other intentional injuries
ALCOHOL DEPENDENCE • Sustained drinking may result in alcohol dependence, a syndrome characterized by impaired control over drinking, high alcohol tolerance, and physical withdrawal symptoms. • Once dependence is present, it impairs a person’s ability to control the frequency and amount of drinking. • Alcohol dependence has many different contributory causes including genetic vulnerability, but it is a condition that is contracted by repeated exposure to alcohol: the heavier the drinking, the greater the risk.
Why alcohol is no ordinary commodity: Relations among alcohol consumption, mediating variables and consequences
NO ORDINARY COMMODITY • Because of its physical toxicity, intoxicating effects, and dependence potential, alcohol is not a run-of-the-mill consumer substance. • Public health responses must be matched to this complex vision of the dangers of alcohol as they seek better ways to respond to population-level harms.
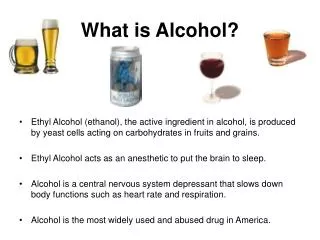
Economic development status and alcohol consumption (based on population weighted averages of 182 countries)
Patterns of drinking 1.00 to 2.00 2.00 to 2.50 2.50 to 3.00 3.00 to 4.00 Patterns of drinking throughout the world
ALCOHOL CONSUMPTION IN DIFFERENT WORLD REGIONS* * population weighted averages ** 1= low level of risk, 4= high level of risk associated with a country’s predominant pattern of drinking
Adult per capita consumption in selected WHO Regions: Africa D (e.g., Nigeria, Algeria), Africa E (e.g., Ethiopia, South Africa), Eastern Mediterranean B (e.g., Iran, Saudia Arabia).
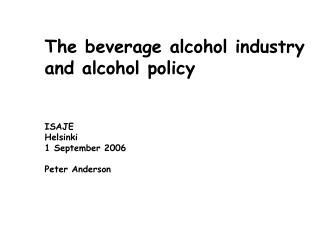
THE GLOBAL BURDEN OF ALCOHOL CONSUMPTION • Alcohol-related death and disability accounted for 4.0% of the global burden of disease, quantified according to the impact of premature deaths and disability in a population. • Alcohol was ranked as the fifth most detrimental risk factor of 26 examined; alcohol accounted for about the same amount of disease as tobacco. • In developed countries, alcohol was the third most detrimental risk factor, accounting for 9.2% of all burden of disease. In emerging economies like China, alcohol was the most detrimental risk factor. • Overall, injuries accounted for the largest portion of alcohol-attributable disease burden. (Murray & Lopez, 1996; Ezzati et al., 2002).
Leading risk factors as causes of disease burden = alcohol, drugs, tobacco Developing countries Developed countries High Mortality LowMortality 1UnderweightAlcoholTobacco 2Unsafe sex Blood pressure Blood pressure 3Unsafe water TobaccoAlcohol 4Indoor smoke UnderweightCholesterol 5Zinc deficiency Body mass index Body mass index 6Iron deficiency Cholesterol Low fruit & veg. intake 7Vitamin A deficiency Low fruit & veg intake Physical inactivity 8 Blood pressureIndoor smoke - solid fuels Illicit drugs 9 TobaccoIron deficiency Unsafe sex 10 CholesterolUnsafe water Iron deficiency 11 AlcoholUnsafe sex Lead exposure 12 Low fruit & veg intake Lead exposure Childhood sexual abuse
ALCOHOL CONSUMPTION TRENDS AND PATTERNS OF DRINKING Alcohol consumption varies enormously, not only among countries, but also over time and between different population groups. Two aspects of alcohol consumption are of particular importance for comparisons across populations and across time. • Total alcohol consumption in a population is an indicator of the number of individuals exposed to high amounts of alcohol. Adult per capita consumption is related to the prevalence of heavy use, which in turn is associated with the occurrence of negative effects. • Variations in drinking patterns (the quantity, frequency and timing of alcohol use) affect rates of alcohol-related problems, and have implications for the choice of alcohol policy measures.
ALCOHOL CONSUMPTION TRENDS • Recorded alcohol consumption is highest in the economically developed regions of the world. Western Europe, Russia and other (non-Moslem) parts of the former USSR now have the highest per capita consumption levels, but Latin American levels are not far behind • Recorded consumption is generally lower in Africa and parts of Asia, and is particularly low in Moslem states and the Indian subcontinent. • Sales data from established market economies show a slight overall decrease in alcohol consumption in recent years, as well as converging trends in traditional high consumption and low consumption countries. (WHO, 1999)
Population Group Differences • There are striking gender differences in whether a person drinks, with men more likely to be drinkers and women abstainers. • Among drinkers, men drink ‘heavily’ (i.e., to intoxication, or large quantities per occasion) much more often than women. • Abstinence and infrequent drinking are more prevalent in older age groups, and frequent intoxication is more prevalent among young adults. Abstinence is the norm in most African countries. • Most of the alcohol in a society is consumed by a relatively small minority of drinkers. • When alcohol consumption levels increase in a country, there tends to be an increase in the prevalence of heavy drinkers.
DRINKING PATTERNS • Countries and population groups vary in the extent to which drinking to intoxication is a characteristic of the drinking pattern. They also differ in how intoxicated people get, and how people behave while intoxicated. • In the southern European countries, approximately one out of ten drinking occasions lead to a state of intoxication among adolescents, whereas the majority of drinking occasions in the most northern European countries result in intoxication (Hibell et al., 1997, 2000).
Alcohol, No Ordinary Commodity:Part II Effective Alcohol Policies:A Consumer’s Guide
Prevention Strategies Reviewed and Evaluated • Pricing and Taxation • Regulating Physical Availability • Altering the Drinking Context • Education and Persuasion • Regulating Alcohol Promotion • Drinking-Driving Countermeasures • Treatment and Early Intervention
Ratings of 32 Policy-relevant Prevention Strategies and Interventions • Evidence of Effectiveness – the quality of scientific information • Breadth of Research Support – quantity and consistency of the evidence • Tested Across Cultures, e.,g. countries, regions, subgroups • Cost to Implement and Sustain – monetary and other costs aRating Scale: 0, +, ++, +++, (?) b Rating Scale: Low, Moderate, High
Policy High taxes, prices Assumption Reduce demand by increasing economic cost of alcohol relative to alternative commodities Assumptions Underlying Pricing and Taxation Policy Options
Pricing and Taxation Evidence suggests that: • People increase their drinking when prices are lowered, and decrease their consumption when prices rise. • Adolescents and problem drinkers are no exception to this rule. • Increased alcoholic beverage taxes and prices are related to reductions in alcohol-related problems. • Alcohol taxes are thus an attractive instrument of alcohol policy because they can be used both to generate direct revenue and to reduce alcohol-related harm. • The most important downside to raising alcohol taxes is smuggling and illegal in-country alcohol production. • Behavioral economic principles apply to discount drink policies, price advertising, differential taxes on different alcohol products (e.g., alcolpops)
Policy Restrictions on time, place, and density of alcohol outlets Assumption Reduce demand by restricting physical availability – increase effort to obtain alcohol Assumptions Underlying Restrictions on Alcohol Availability
Regulating Alcohol Availability • Changes in availability can have large effects in nations or communities where there is popular support for these measures. • The cost of restricting alcohol availability is cheap relative to the costs of health consequences related to drinking, especially heavy drinking. • The most notable adverse effects of availability restrictions include increases in informal market activities (e.g., cross-border purchases; home production, illegal imports).
Regulating Alcohol Availability Through Minimum Legal Purchase Age (MPLA) • In 1984 the US Congress passed the National Minimum Purchase Age Act, which encouraged states to adopt the age 21 purchase standard • The number of young people who died in a crash when an intoxicated young driver was involved has declined by almost 63%
Modifying the Drinking Context Many prevention measures seek to re-define the contexts or change the environments where alcohol is typically sold and consumed (e.g., bars and restaurants), under the assumption that such changes can reduce alcohol-related aggression and intoxication . Options include training bar staff, imposing voluntary house policies to refuse service, enforcement of regulations, community mobilization to influence problem establishments
Regulating alcohol promotion • The marketing of alcohol is a global industry. • Alcohol brands are advertised through television, radio, print, point-of-sale promotions, and the Internet. • Exposure to repeated high-level alcohol promotion inculcates pro-drinking attitudes and increases the likelihood of heavier drinking. • Alcohol advertising predisposes minors to drinking well before legal age of purchase. • Advertising has been found to promote and reinforce perceptions of drinking as positive, glamorous, and relatively risk-free.
Stamp of Approval 4:06 A.M. WE GET PAST OUR SIXTH DOORMAN OF THE EVENING SEE WHERE IT TAKES YOU
Policy Regulating alcohol marketing and advertising Assumption Reducing exposure to social modeling of excessive drinking will prevent underage drinking Assumption Underlying Regulation of Alcohol Marketing Policy Options
Regulating alcohol promotionIndustry Self-regulation Codes • Self-regulation tends to be fragile and largely ineffective. • These codes may work best where the media, advertising, and alcohol industries are all involved, and an independent body has powers to approve or veto advertisements, rule on complaints, and impose sanctions. • Few countries currently have all these components.
Policy Drink-driving countermeasures Assumption Reduce drink driving though deterrence, punishment and social pressure Assumptions Underlying Drink-driving Policy Options