Download
1 / 5
50 likes | 74 Vues
This proposal aims to improve patient discharge and assessment processes through system agreement, community support infrastructure, joint funding, and addressing conflicting priorities. It includes the implementation of the Home to Assess model and a residential reablement pathway.

E N D
Discharge to Assess Helen Krysinski
Issues and enablers • System agreement and buy in- understanding D2A • Current community infrastructure to support D2A- commissioned providers • Joint funding agreement • Conflicting priorities and influence to change • Pathway 1 provider- fragile • Structural stakeholder changes – ESNEFT/ECC/Alliance/IBCF reporting • Unpicking the current pathway avoiding duplication of services • Community social care team with capacity to ensure rapid flow through the proposed D2A pathways. • Organic model with expanding scope
Pathway 1/2 – Home to Assess model implementation - Home to assess. (requires approval and funding) Home to Assess will provide a service to pull patients from the acute hospital from ward level. Ensure same day availability of services to discharge patients to their own home. Provide with a wrap around assessment and support for 5 days. The service will then handover the continuity of care seamlessly to the appropriate provider. • Pull from hospital wards- same day discharge • Full assessment same day at home • Wrap around support provided –nurse ,therapies and care workers for 5 days in the home • Goals set for rapid rehabilitation/reablement and continued assessment against goals • Full social care assessment • Referral and signposting to ongoing services- continued reablement short term ,voluntary services and medium to long term care provision. • Maximising independence and reducing the long term care needs of the adult. • Can do ethos with patients at the centre.
Pathway 2/3 residential reablement and sourcing of long term needs. For patients who are unable to return home safely but require a short period of residential reablement and rehabilitation. The aim is for all patients to return to their own home or to suitable long term accommodation. • Identify 20-30 beds in current residential/care homes to accommodate transfer of patients directly from the acute hospital. • Implementing a pull model facilitated by a coordinating therapist who will work across the hospital and community setting. • Same day discharge • Full assessment and plan of care to promote independence • Wrap around support provided –therapies, social care and care workers for up to 2 weeks • Goals set for rapid rehabilitation/reablement and continued assessment against goals • Support and review by a doctor to reduce the risk of failure due to limited primary care provision • Referral and signposting to ongoing services- continued reablement ,voluntary services and medium to long term sourcing of care provision. • Maximising independence and reducing the long term care needs of the adult. • No assessments in the acute hospital
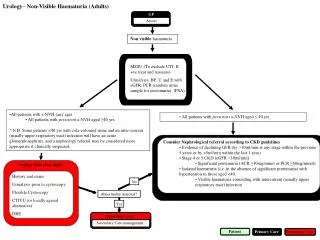
Patient no longer requires acute hospital intervention Pathway 0 Pathway 1 Pathway 2 Pathway 3 Safe to return home with moderate short term support ? Patients with rehab potential but unlikely to return to their original place of residence. Would improve function and reduce long term care needs Needs can be met safely at home/further rehab reablement. Pull from the acute Consider short stay whilst sourcing long term placement N0 additional ongoing care needs Y N Home Pull from the acute Focused intervention and support to return home or to source long term care up to 2 weeks in the facility Focused intervention and support in the home up to 5 days. Discharge home , restart existing care or support package. Refer to voluntary services as needed. 5 Day focused assessment and reablement/rehab. Commissioned providers : 2 weeks Reablement and rehabilitation in the home- only extended to 6 weeks in exceptional circumstances- refer to services for ongoing needs Rehabilitation /care in community bed specialist input is required . CHC assessment if appropriate Proposed residential discharge pathway Home to assess provision