Download
1 / 78
820 likes | 1.51k Vues
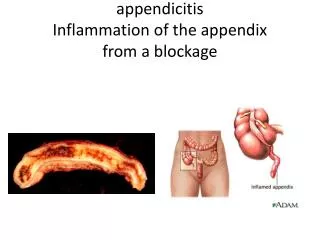
Appendix removed from patient with acute appendicitis. Note the rough, shaggy material (arrows) on the surface due to deposition of fibrin and inflammatory cells. Appendix with acute inflammatory response Normal Appendix

E N D
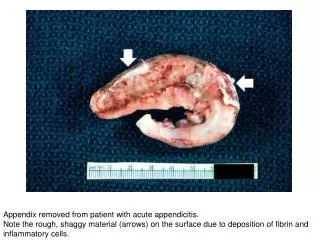
Appendix removed from patient with acute appendicitis. Note the rough, shaggy material (arrows) on the surface due to deposition of fibrin and inflammatory cells.
Appendix with acute inflammatory response Normal Appendix Note the abundant blue-staining lymphoid tissue beneath the mucosal layer and the absence of blue-staining cells in the submucosal layer in the normal appendix. Compare this with the extensive distribution of cells in the appendix with acute appendicitis. The blue color is due to the presence of many inflammatory cells, although at this low power the individual cells cannot be specifically identified.
Appendix with acute inflammation Note there are only remnants of mucosal tissue identifiable along the luminal border There is an extensive infiltration of leukocytes. Notice that the surface is rough and has deposits of fibrin.
1: Serosal surface of the appendix 2: Submucosal center with remnants of a lymphoid nodule. Surrounding this lymphoid nodule are masses of leukocytes which should not be present in a normal appendix.
Arrow: A small area of normal mucosal epithelium. This area is surrounded by areas of ulceration with an inflammatory infiltrate of lymphocytes and neutrophils.
Arrows: Loss of normal mucosal epithelium and the inflammatory infiltrate The principal inflammatory cell in this case of acute appendicitis is the neutrophil.
Open abdominal cavity of a patient with acute appendicitis There has been rupture of the appendix with spillage of the intestinal contents into the abdominal cavity. This spillage resulted in an “acute abdomen” and widespread inflammation throughout the abdominal cavity. Note the roughened surface of the mesenteric tissue (arrow) due to the deposition of fibrin over much of the surface.
Another example of peritonitis Note the fibrinosuppurative exudate covering the abdominal organs
Acute lobar pneumonia The left lung is affected with pneumonia (arrows). It has whitish discoloration and appears swollen compared to the more pink-staining normal lung (lower right and left had portions of the photo).
Cut section of lung with acute lobar pneumonia Note the whitish discoloration of the tissue in the upper lobe (arrows) compared to the normal collapsed and pink-staining lung lobe in the left-hand portion of the photo. The white discoloration is due to infiltration of leukocytes, primarily neutrophils. Note that only one lobe of the lung is involved in this patient.
Right lung of the same patient This lung shows complete consolidation with a marked infiltration of neutrophils throughout the tissue, giving a whitish discoloration. This is an advanced case of lobar pneumonia with extensive necrosis which obviously did not resolve, thus resulting in the death of the patient. Note the extensive black pigment due to anthracosis.
1: Markedly thickened pleura, indicating an inflammatory process that has been ongoing for days 2: A small, wedge-shaped segment of normal lung which is somewhat compressed due to artifact 3: A large, wedge-shaped segment of lung with lobar pneumonia, which appears very dense due to extensive cellular infiltrate 4: A greatly thickened pleural space between these two lobes due to deposition of fibrinous exudate
Interpleural space between the two lobes 1: Thickened pleura with extensive fibrin deposits 2: The affected lung lobe 3: Extensive fibrin deposits in the interlobar space
Junction of the pleura (1) with the pneumonic lung parenchyma Arrows: outline of alveolar structures The mass of cells infiltrating this tissue consist almost exclusively of neutrophils (PMNs).
Junction of pleura (1) with parenchyma Note the alveoli (2) filled with PMNs, alveolar macrophages, and fibrin The dark red-stained material (3) is fibrin in the pleura. There are RBCs trapped in the fibrinous pleuritis as well.
Alveoli filled with exudate The alveolar walls (arrows) are barely visible. The alveoli are filled with PMNs, fibrin, and edema fluid. This is a severe acute inflammatory response but the structure of the alveoli remains intact. This tissue is able, with proper treatment, to completely resolve this inflammatory response. Since there has not been necrosis, this lung could completely recover normal function (resolution).
Lung with multiple abscesses Arrows: individual lung abscesses
1: Multiple focal lesions 2: Lesion with a pale center, indicating loss of parenchymal tissue. This is typical of abscess formation in the lung and represents liquefaction necrosis. This is bronchopneumonia since the distribution is along the bronchi and the terminal airway distribution throughout the lung. Note that there are some areas that appear completely normal, having a normal-staining appearance. Other areas are much darker (3), indicating a heavy cellular infiltrate.
1: Wall of the abscess 2: Liquefaction necrosis in the center of the abscess 3: The remaining lung tissue has extensive infiltration into the alveoli. The abscess has destroyed a portion of the lung, but other areas of the lung where the structure has been retained could recover normal function.
Lung with bronchopneumonia Note that the alveolar structure of this tissue, which is in the region of a terminal bronchiole (1), has been retained despite the massive infiltration of inflammatory cells. These inflammatory cells are primarily neutrophils.
1: A terminal bronchiole in which the mucosal lining has been almost completely destroyed There is extensive neutrophilic infiltration throughout this tissue.
Central portion of an abscess Note the absence of any parenchymal tissue due to extensive neutrophilic infiltration with liquefaction necrosis of the parenchymal tissue. Masses of leukocytes (primarily neutrophils), fluid, and necrotic debris within an abscess form what is referred to as “purulent material” or “pus”. The blue-staining mass in the center of this abscess (arrow) represents colonies of bacteria.
Lymph Node Note the rather pale pink color of the tissue with dark-staining cells found in only a few scattered areas. These darker cells represent the original lymphocytes cells of this lymphoid organ.
Lymph Node Illustrates a paucity of lymphocytes as well as numerous, pale-staining nodules (arrows) throughout the tissue
The small nodules (arrows) seen in the previous image Close examination reveals they are composed of macrophages (epithelioid macrophages). These small granulomas form multiple series of reaction centers throughout the lymph node. Note the remaining lymphocytes surrounding the granulomas.
Single granuloma Arrows: Individual macrophages that make up the bulk of the tissue In this case, there is an absence of necrosis in the center.
1: Multinucleated giant cell 2: In the center of this foreign-body containing giant cell there is a small asteroid body. No functional significance.
Note that the lesion appears solid and has a whitish coloration, indicating considerable fibrous connective tissue. This is a healed granuloma due to primary Tb in the lung. There are smaller focal lesions adjacent to the major mass. In addition, notice the extensive anthracosis.
Multiple large nodules (1) with pale eosinophilic centers surrounded by a rim of blue-staining tissue. In addition to the large nodules, there are several smaller nodules (2) throughout the slide.
Tb Granuloma Central core of caseation necrosis (1) encircled by a rim of epithelioid macrophages and lymphocytes (2). Langhans type multinucleated cells are present, but difficult to see (3).
Granuloma 1: Necrotic core 2: Epithelioid macrophages 3: Langhans’ type giant cells Note the small lymphocytes, characterized by their distinctly blue-staining nuclei. Other cells include fibroblasts and occasional neutrophils.
Tb Granuloma Acid-fast bacilli (arrows)
Lung and Pleura Arrows: Hemorrhages Arrows: Small focal lesions throughout parenchyma
These granulomas surround blood vessels. Note RBC in lumen (arrow).
Taken under partially polarized light to demonstrate the birefringent particles within the granulomas (1) These granulomas are adjacent to blood vessels (2). Fully polarized light Shows numerous birefringent particles
Acute Fibrinous Pericarditis The pericardium on this heart has been reflected back (arrows). The surface of the heart is rough due to the deposition of fibrin on the epicardial surface of the heart and on the inner surface of the pericardium.
Heart with pericardium removed Most of epicardial surface is covered with fibrinous deposits. There are a few glistening areas of exposed normal epicardial tissue.
Arrows: Dark-red staining fibrin deposits on the inner surface The pericardium is much thicker than normal and there are numerous inflammatory cells within the pericardial tissue.
Arrows: Fronds of fibrin extending from the surface of the pericardium
Fibrin (red amorphous material) on the surface of the pericardium (1) Note the reactive mesothelial cells on the surface of the pericardium (arrows) and the inflammatory cells within the pericardium.
Stomach containing an ulcer Note the folded pink gastric mucosa that extends up to the edge of the ulcer (arrows)
The ulcer after it has been transected 1: Edge of the mucosa 2: The thick fatty tissue which makes up the base of the ulcer (3)
Transected ulcer 1: Normal gastric epithelial cells of the mucosa 2: Crater of the ulcer; note the absence of cells
Margin of the ulcer 1: Intact epithelium 2: Ulcerated region with no epithelium There are numerous inflammatory cells.
Base of the ulcer 1: Fibrinopurulent membrane overlying the ulcerated surface 2: The ulcerated surface contains granulation tissue and inflammatory cells.
Arrows: Ulcer Base; note the lack of epithelium 1: Exhuberant inflammatory response consisting primarily of fibrin, adherent gastric secretions, and PMNs The surface of the ulcer bed is covered with this fibrinopurulent exudate.
Plump, activated fibroblasts and endothelial cells (arrows) within the granulation tissue that makes up the base of the ulcer. There are inflammatory cells (primarily lymphocytes) in this region as well.
Serosal Surface Base Healing reaction at the ulcer base Note the fibrous connective tissue within the wall of the stomach and the layer of inflammatory exudate on the surface of the ulcer (arrow)