Download
1 / 43
440 likes | 548 Vues
Learn about the antibiotics-first approach in treating uncomplicated acute appendicitis, comparing it with the traditional appendicectomy method. Explore the effectiveness, outcomes, and limitations of antibiotic therapy in this comprehensive summary.

E N D
Antibiotics-first approach in uncomplicated acute appendicitis JOINT HOSPITAL SURGICAL GRAND ROUND WONG YIM PING TUEN MUN HOSPITAL 23rd April, 2016
Outline • Background and introduction • Definition • Literature review and appraisal • Summary
Acute appendicitis • One of the commonest cause of acute abdomen • Lifetime incidence 7% in the US population[1] • In Hong Kong 2492 appendicectomies were performed in year 2014-2015[2] [1] Addiss DG, Shaffer N, Fowler BS, Tauxe RV. The epidemiology of appendicitis and appendectomy in the United States. Am J Epidemiol. 1990;132:910–25. [2] SOMIP reprt July 2014 –June 2015
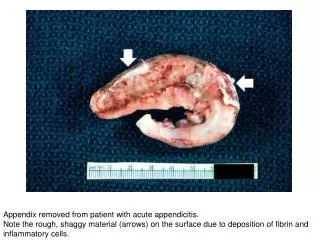
Conventional teaching • Appendicectomy for uncomplicated appendicitis • Prevent progression to perforation and other complications • Appendicectomy is a surgery of low morbidity and mortality
Antibiotics first approach • Antibiotic therapy • Supportive care • Careful observation • +/- appendicectomy
Uncomplicated acute appendicitis • No universal consensus • = Simple acute appendicitis
Sallinen, V., Akl, E. A., You, J. J., Agarwal, A., Shoucair, S., Vandvik, P. O., Agoritsas, T., Heels-Ansdell, D., Guyatt, G. H. and Tikkinen, K. A. O. (2016), Meta-analysis of antibiotics versus appendicectomy for non-perforated acute appendicitis. Br J Surg, 103: 656–667. doi: 10.1002/bjs.10147
Key points • Five studies included, total 1116 adult patients • Single-center or multicenter randomized trials • All were conducted in the Europe • Participant: patients with suspected uncomplicated acute appendicitis ( clinical +/- radiological)
Key points • Intervention : • 3rd generation cephalosporin IV fluoroquinolone and tinidazole PO • Carbopenem IV fluoroquinolone + metronidazole PO • Amoxicillin plus clavunalic acid IV or PO • Duration of treatment 8-15 days • No pre-specified cross over criteria in most studies
Key points • Control: open or laparoscopic appendicectomy • Outcomes measure: • Appendicectomy rate within index admission • Success of treatment • Post intervention complications • Recurrence • Length of stay • Length of sick leave • Pain( VAS or medications use)
Outcome measures • Rate of appendicectomy within 1 month • Major complications • Minor complications • Recurrence of appendicitis • Length of hospital stay • Length of sick leave
Major complications • Clavien- Dindo complications grade III or above • Appendiceal perforation • Deep infections • Incisional hernias • Adhesive bowel obstruction not requiring intervention
Minor complications • Superficial wound infections • Diarrhea • Abdominal discomfort
Recurrence of appendicitis • Confirmed or suspected recurrence of appendicitis between 1 month and 1 year
Pain measure • Not included as inconsistent measurement of pain
Conclusion • Length of hospital stay is shorter in the appendicectomy group (p<0.001)
Limitation of current evidence • Poor study design • Low enrollment rate, ? Selection bias • Difficulty in establishment of diagnosis • Poor generalizability • High crossover rate
Hansson J, Korner U, Khorram-Manesh A, Solberg A, Lundholm K. Randomized clinical trial of antibiotic therapy versus appendicectomy as primary treatment of acute appendicitis in unselected patients. Br J Surg 2009; 96: 473–481.
Summary • Large multicenter high quality randomized trials are needed before the antibiotics-first approach could be considered comparable to appendicectomy
Summary • Appendicectomy remains the standard treatment for acute appendicitis • Non operative management reserves to selected group of patients
The appendectomy remains the treatment of choice for acute appendicitis. Antibiotic therapy is a safe means of primary treatment for patients with uncomplicated acute appendicitis, but this conservative approach is less effective in the long-term due to significant recurrence rates. (Recommendation 1A).
Reference • Sallinen, V., Akl, E. A., You, J. J., Agarwal, A., Shoucair, S., Vandvik, P. O., Agoritsas, T., Heels-Ansdell, D., Guyatt, G. H. and Tikkinen, K. A. O. (2016), Meta-analysis of antibiotics versus appendicectomy for non-perforated acute appendicitis. Br J Surg, 103: 656–667. doi: 10.1002/bjs.10147 • Eriksson S, Granstrom L. Randomized controlled trial of appendicectomy versus antibiotic therapy for acute appendicitis. Br J Surg 1995; 82: 166–169. • Salminen P, Paajanen H, Rautio T, Nordstrom P, Aarnio M, Rantanen T et al. Antibiotic therapy vs appendectomy for treatment of uncomplicated acute appendicitis. JAMA 2015; 313: 2340–2349. • Styrud J,Eriksson S,Nilsson I, Ahlberg G, Haapaniemi S, Neovius G et al. Appendectomy versus antibiotic treatment in acute appendicitis. A prospective multicenter randomized controlled trial. World J Surg 2006; 30: 1033–1037.
Reference • Svensson JF, Patkova B, Almstrom M, Naji H, Hall NJ, Eaton S et al. Nonoperative treatment with antibiotics versus surgery for acute nonperforated appendicitis in children. Ann Surg 2015; 261: 67–71. • Vons C, Barry C, Maitre S, Pautrat K, Leconte M, Costaglioli B et al. Amoxicillin plus clavulanic acid versus appendicectomy for treatment of acute uncomplicated appendicitis: an open-label, non-inferiority, randomised controlled trial. Lancet 2011; 377: 1573–1579. • Hansson J, Korner U, Khorram-Manesh A, Solberg A, Lundholm K. Randomized clinical trial of antibiotic therapy versus appendicectomy as primary treatment of acute appendicitis in unselected patients. Br J Surg 2009; 96: 473–481.
Antibiotic • Common pathogens: Enteric gram- negative bacilli, anaerobes, enterococci • Mono therapy with a beta- lactam/ beta- lactamase inhibitor, i.e. Ampicillin- sulbactam, Piperacillin- tazobactam, Ticarcillin- clavulanate • Combination third generation cephalosporin plus metronidazole, i.e. Ceftriaxone plus metronidazole
Alternative empiric regimens • Combination fluoroquinolone plus metronidazole, i.e. Ciprofloxacin or levofloxacin plus metronidazole • Mono therapy with a carbapenem, i.e. Imipenem- cilastatin, meropenem, doripenem, ertapenem
Surg: 9 Abx: 6 Laparoscopic vs open
CTsensitivity • For diagnosis • For differentiating complicated vs uncomplicated
Complicated acuteappendicitis • Appendiceal maximal diameter (>10 mm), periappendiceal fat infiltration, and ascites on CT findings and CRP (>5 mg/dL) ---------Min BW. Change in the Diagnosis of Appendicitis by Using a Computed Tomography Scan and the Necessity for a New Scoring System to Determine the Severity of the Appendicitis. Annals of Coloproctology. 2015;31(5):174-175. doi:10.3393/ac.2015.31.5.174.
Risks factors of recurrent appendicitis • Male gender ------Lien WC1, Lee WC, Wang HP, Chen YC, Liu KL, Chen CJ. Male gender is a risk factor for recurrent appendicitis following nonoperative treatment. World J Surg. 2011 Jul;35(7):1636-42. doi: 10.1007/s00268-011-1132-5.