Download
1 / 11
140 likes | 454 Vues
Acute Appendicitis Tintinalli C hap. 78. Nicholas Cardinal, DO. Pathophysiology. Obstruction of appendiceal lumen Food matter Adhesions Lymphoid hyperplasia Mucosal secretion Causes increased intraluminal pressure Vascular compromise

E N D
Acute AppendicitisTintinalliChap. 78 Nicholas Cardinal, DO
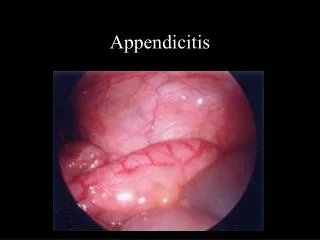
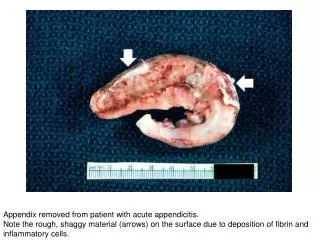
Pathophysiology • Obstruction of appendiceal lumen • Food matter • Adhesions • Lymphoid hyperplasia • Mucosal secretion • Causes increased intraluminal pressure • Vascular compromise • Causes breakdown of epithelial mucosa and bacterial invasion • Inflammatory response • Further increases intraluminal pressure • Eventually leads to arterial stasis and tissue infarction
Innervation • Luminal distention • Triggers visceral afferent fibers entering at T10 • Vague, poorly localized periumbilical or epigastric pain • Inflammation of serosa and adjacent structures • Triggers somatic pain fibers • Localized to RLQ • Anatomic Variability • Retrocecal (26%) • Flank pain • RUQ • Pregnant women • Retroileal • Testicular pain • Pelvic • May irritate bladder or rectum causing suprapubic pain, pain with urination, or feeling of a need to defecate
Symptoms • Vague abdominal pain with localization • 64% sensitive, 82% specific • Anorexia • 68% sensitive, 36% specific • N/V • 50% sensitive, 45% specific • Rebound tenderness • 63% sensitive, 69% specific • Guarding • 74% sensitive, 57% specific • Rigidity • 27% sensitive, 83% specific • Fever • 67% sensitive, 79% specific
Physical Exam • McBurney’s point • May have rectal or flank tenderness if pelvic or retrocecal • Rovsing sign • Palpation of LLQ produces RLQ pain • Psoas sign • Patient in left lateral decubitus • Extend right leg at hip • Obturator sign • Passive flexion of hip & knee with internal rotation of hip
Diagnostics • CBC • 70-90% sensitive, low specificity • Urinalysis • Abnormal in 19-40% • Plain Radiographs • Limited diagnostic value • Abnormal in 24-95% • Look for appendiceal gas, fecalith, localized paralytic ileus, blurred right psoas muscle, free air
Diagnostics • Graded Compression Ultrasound • 94.7% sensitive, 88.9% specific • Inflamed appendix cannot be compressed • Findings • Diameter > 6mm • Presence of appendicolith • Periappendiceal abscess • Doppler may show hyperemia • Limitations • Retrocecal • Ruptured appendix = normal diameter
Diagnostics • CT • Appears to change management decisions and decrease unnecessary appendectomies in women • Greater sensitivity (96%), accuracy (94%), and negative predictave value (95%) than ultrasound • Findings • Pericecal inflammation • Abscess • Periappendicealphlegmon • Fluid collections • Localized fat stranding
Special Populations • Very young • High misdiagnosis rate • High perforation rate • Communication difficulty • Atypical symptoms • Concurrent respiratory symptoms • Gastroenteritis • Lethargy, inactivity, hypothermia • Elderly • Late presentation with an advanced course • Misdiagnosis can exceed 50% • Incidence of perforation 40-70% • Mortality rate in patients > 70 ~ 30% • Pregnant • Most common extrauterine surgical emergency • Fetal mortality rate increases up to four times if complicated by perforation and peritonitis • AIDS • Delayed dianosis • Frequency of GI symptoms • No leukocytosis • Higher incidence of perforation
Management • NPO • IV fluids • Preoperative antibiotics • Cover for anaerobes, enterococci, and gram-negative’s • Zosyn 3.375 grams IV • Unasyn 3 grams IV • Analgesics • Surgical consult