Download
1 / 56
560 likes | 638 Vues
This article explores the different levels of intellectual disability, assessment considerations, coexisting issues, and the impact of cultural influences. Considerations for assessment, the Flynn effect, and communication challenges are delved into, highlighting the role of psychologists in diagnosing and supporting individuals with intellectual disabilities.

E N D
Intellectual Disability and Clinical Psychology Marleen Verhoeven Consultant Clinical Psychologist Regional Dual Disability Service Counties Manukau DHB
Intelligence David Wechsler: "the global capacity of the individual to act purposefully, to think rationally, and to deal effectively with his environment."
What is Intellectual Disability? Intellectual Disability is characterized by deficits in general mental abilities such as reasoning, problem-solving, planning, abstract thinking, judgment, academic learning and learning from experience DSM-V
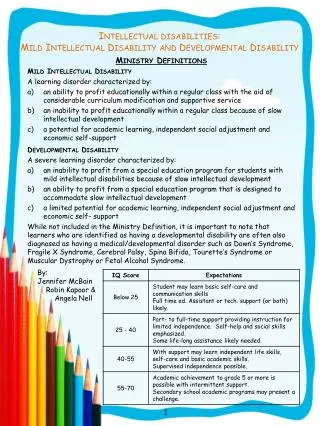
A person with mild intellectual disability • Often not identified as “retarded” • May marry and hold a job • May only need help at times of crisis, e.g. social or economic stress • May have attended special school, and live and work semi-independently with some extra supports • Brain pathology uncommon • IQ 50/55-70: 85%
A person with moderate intellectual disability • Often capable of independence but needs supervision • Able to communicate, follow interests and manage simple tasks • Brain pathology a possibility • IQ 35/40-50/55: 10%
A person with severe intellectual disability • Needs considerable help with ADL’s but often can wash and maintain continence • Physical disability and motor problems common (e.g. Cerebral Palsy) • Limited communication, often no speech • Brain pathology common • IQ 20/25-35/40: 3.5%
A person with profound intellectual disability • Needs extensive full time care • Minimal communication • Brain pathology likely • IQ <20/25: 1.5%
Common coexisting issues • Physical, sensory disability • Pervasive Developmental Disorder • Autism Spectrum Disorder (ASD) • ADHD • Alzheimer’s Disease • Mental illness (3-4x general popn) • Trauma history • Poor coping skills
Considerations for assessment • Labelling or meeting needs? • Flynn effect • Cultural influence • Reasons for assessment • Informed consent • Communication issues • Diagnostic overshadowing • Effort testing
The Flynn effect • IQs on the Wechsler tests rose steadily throughout the 20th century at the rate of about .3 IQ points a year • Following re-norming, an average drop of 5.6 IQ points WISC-R > WISC-III • About half of the children with IQs of <75 have an IQ of 71-75 • In 80s more children diagnosed with ID, pointing to the risk of labelling people • A similar trend has been observed following WAIS-IV
Cultural influence • USA has a high percentage of minority children in ID programmes • NZ has a high percentage of underachieving children in comparison to international statistics, especially within Maori and Pacific Island cultures • This has resulted in a move away from labelling intellectual disability during the developmental years
Labelling or meeting needs? • Statistics NZ 2001: 2% children, 1% adults have a known intellectual disability • Bell shaped curve: 2.2% • Barriers to diagnosis: • Access to psychologists • Cultural issues • Language barriers • Poverty • Lack of insight • Lack of advocacy • Other disability e.g. ASD, sensory
Considerations • Psychologists are the only professional group qualified to diagnose ID • People with an intellectual disability are one of the most vulnerable and disempowered groups in our society • We carry a responsibility to act in their best interest
Reasons for assessment • Referral to a NASC (Needs Assessment and Service Co-ordination) e.g. Taikura Trust • Court ordered e.g. IDCCR Act (Intellectual Disability Compulsory Care and Rehabilitation Act), witness in Court, PPPR Act (Protection of Personal Property and Rights Act) • RIDCA is intensive service co-ordination for people with an ID who have criminally offended and are going though the Court process or are already under the IDCCR Act
NASC Ministry of Health, DSS contracted agency which: • Requires evidence of ID (or other disability if agency holds this contract) • Undertakes needs assessment • Coordinates services i.e. Behaviour Support, Carer Support, Supported Independent Living, Residential Services • Contracts these services out to Ministry of Health funded community agencies
Informed consent • An adult is assumed competent to consent to treatment / assessment unless they have a Welfare Guardian or Enduring Power of Attorney (PPPR Act) or receive compulsory treatment (Mental Health Act, IDCCR Act)
Communication issues • “You are NOT going to the pool” • “You will be going to the pool tomorrow” • “I do not believe that you are not going to the pool” • “How was the pool?” • “Did you hear voices (at the pool)?”
Communication issues • Difficulties with insight, ability to express, putting things in a logical order, prioritising • Keep vocabulary simple, use their own words • Difficulties with abstract thought – keep communication concrete and factual • Suggestibility • Take time and respect the person’s opinion: avoid short cuts!
Diagnostic overshadowing • When a person's presenting symptoms are put down to their known condition, rather than seeking another cause • Person with ASD in MH service: “the devil made me do this” • Person with ID experienced sexual abuse but professionals presumed behaviours were down to ID or psychosis (inappropriate sexual behaviours; asking if her niece had been raped).
Effort testing • The Test of Memory Malingering, TOMM: in spite of it’s name is a test of effort • It measures poor effort due to e.g. tiredness, undue anxiety, depression, illness as well as motivational factors • There are other effort tests, not all suited to ID • Arguably use TOMM before each psychometric test
AAIDD / DSM-IV-TR Three criteria of intellectual disability: • Significant sub-average intellectual functioning (IQ 70 or below), and; • Concurrent deficits or impairments in present adaptive functioning, and; • Low functioning apparent during the developmental years, prior to the age of 18 years.
IDCCR Act 2003 • We have legislation that clarifies criteria that need to be met for the diagnosis • Sections 7 and 8 • Definition of ID consistent with DSM-IV-TR (DSM V?)
1. Intellectual functioning Recommended intelligence tests: • Wechsler Intelligence Scales • WISC-IV • WAIS-IV • Stanford Binet Intelligence Scale (5th edition)
Tests not recommended • Wechsler Abbreviated Scale of Intelligence – please use only in research. Clinically this impacts upon the ability to do a full WAIS-IV • Kaufman’s tests are culturally biased to USA context, e.g. American coins, baseball • Slosson Intelligence Test (SIT-III) is a quick estimate of verbal cognitive ability, a screen only, psychometrically weak
Person with limited English • When the person has limited familiarity with the English language, or when they are from a non Anglo-Saxon culture, the standard Wechsler and Stanford Binet tests pose some difficulties • Use of non-verbal tests recommended, with clear explanation of why they were used and what their limits are • Tests may be language free, but they are not culture free
Person with limited English • Make sure a professional translator is present!!! • In past WAIS PIQ recommended, with Test of Non-verbal Intelligence, TONI-C an alternative option • WAIS IV no longer includes PIQ - now broken down into Verbal Comprehension; Perceptual Reasoning; Working Memory; Processing Speed • Ravens SPM – acceptable but norms difficult at low levels. Can help to eliminate ID as diagnosis
Hearing impaired Use interpreter in their own communication style Recommended tests: WAIS PIQ (WAIS IV?) or TONI-C
Person with Physical Disability • Cerebral palsy or other physical disability may significantly affect motor and verbal communication skills. Consider use of: • Peabody Picture Vocabulary Test, PPVT • TONI offers a non-verbal IQ measure
Acquired brain injury during childhood • The individual may meet the 3 criteria for the diagnosis of an intellectual disability and is entitled to supports from NASC (depending on ACC involvement) • Some regions have specialised facilities and resources available to those whose injury is as above, and some intellectual disability services may exclude those whose impairment was caused by injury, particularly if acquired late in the developmental period
Acquired brain injury during childhood • Intellectual functioning profiles may not be typical of an intellectual disability • Typical ID profile exhibits “relatively flat score profiles, with the lowest scores obtained on Arithmetic, Vocabulary, and Coding” (WAIS-III technical manual)
Extremely poor concentration span • Some people may still be testable with brief tests like WASI, TONI-C, TONI-3, Ravens SPM, PPVT
Person unable to be tested • Unspecified ID: severity undetermined • Untestable due to: • Extreme intellectual disability • Extreme behavioural issues • Concurrent severe disability e.g. sensory, autism • Concurrent dementia e.g. chronic mental illness with severe perseveration, catatonia
Person unable to be tested • Do the best you can • Use clinical judgement combined with an adaptive functioning test & developmental history • Review as much material as possible • It’s standard practise for NASC to seek a second opinion • Provide what information you have to the person completing the second opinion
Person mentally unwell • If the person is mentally unwell, wait until they recover wellness. If there are timeframes that make this difficult explain this in a report. You may need to give a provisional opinion with recommendations to revisit it in time, but most importantly do not try to use a psychometric test at this time as it will mean that later testing when the individual is mentally well may be compromised.
IQ: Intelligence Quotient Bell shaped curve Intellectual disability: <2sd 1% – 2.2% of our population
Standard error of measurement • If IQ range includes IQ 70 or below, person is on the cusp and may have an intellectual disability e.g. 68-75 • Use other 2 criteria to determine
Subtest and index scatter • Try and identify the reason: genetic syndrome, ASD, acquired brain injury, mental illness, abuse and neglect, poor educational opportunities, substance abuse, cultural factors… • WISC: 70% of children with specific learning difficulties score lower FSIQ than GAI. General Ability Index has less reliance on WM and PS. However, GAI is not necessarily a more valid estimate of overall cognitive ability than the FSIQ (Pearson, 2005) • If significant scatter, diagnose or not?
Inconsistency between IQ and adaptive behaviour If one or the other is above the cut-off for an intellectual disability, the person does not meet criteria of the diagnosis
Different IQ scores over time • It is commonly assumed that a person can lower their performance on an IQ test, but not achieve higher than their potential. The higher IQ result is therefore more reliable in the absence of another explanation. • A lower IQ score may be due to environmental and personal factors at the time of testing. Furthermore, test results are very dependent upon the respondent applying full effort and engaging with the testing scenario. It may also be due to neurological, other health or psychiatric deterioration. Another cause may be the type of assessment instrument used.
2. Adaptive behaviour How effectively a person copes with common life demands and how well they meet the standards of personal independence expected of someone in their particular age group, socio-cultural background and community setting
2. Adaptive behaviour: DSM-IV-TR “existing concurrently with related limitations in two or more of the following applicable adaptive skill areas: communication, self-care, home living, social skills, community use, self-direction, health and safety, functional academics, leisure, and work” AAMR (1992) and DSM-IV-TR
2. Adaptive behaviour: AAIDD “significant limitations in adaptive behaviour as expressed in conceptual, social, and practical adaptive skills” AAIDD (formerly AAMR, 2002)
2. Adaptive behaviour: DSM-V • Increased focus on adaptive behaviour • To include cultural sensitivity • Intends to be consistent with AAIDD definition • Recommends factor analysis and standard tests
2. Adaptive functioning tests • Vineland Adaptive Behaviour Scales II • Adaptive Behavior Assessment Scale (please note: standard score 4 or below) • Adaptive Behavior Scale – Residential and Community • Diagnostic Adaptive Behaviour Scale (2010) by AAIDD
If “best tests” cannot be used: • Scales of independent behaviour – SIB-R (has a short form for visually impaired) • Practical tests that can provide collateral information (OT type assessment), but utmost caution around making firm diagnoses based on the findings of these alone • Direct observation, multiple informants, questionnaire based on behaviour prior to secure environment, file review of evidence of adaptive behaviour
3. Developmental years The onset is before age 18 years 70%: Aetiology unknown