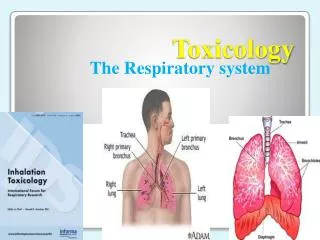
Toxicology conference
320 likes | 492 Vues
Toxicology conference. 2011.12.16 指導醫師:許景瑋醫師 報告者: fellow 1 潘恆之. P resentation. Patient Profile. Name: 趙 o 林 Sex: male Age: 39 years old Chart number: 8767453 He visited our emergent room on 2011/11/04. Chief Complaint. Acute onset of blurred vision lasts for one day. Present Illness.

Toxicology conference
E N D
Presentation Transcript
Toxicology conference 2011.12.16 指導醫師:許景瑋醫師 報告者:fellow 1 潘恆之
Patient Profile • Name: 趙o林 • Sex: male • Age: 39years old • Chart number: 8767453 • He visited our emergent room on 2011/11/04
Chief Complaint • Acute onset of blurred vision lasts for one day.
Present Illness • This 39 y/o gentleman denied hypertension, diabetes mellitus or other systemic diseases. • He had experienced intermittent nausea, vomiting , and progressive anorexia since 11/01. Acute onset of blurred vision , dizziness, headache were noted since 11/04 morning. Besides, he suffered from intermittent bloody stool for 1 years. • No dyspnea, orthopnea, urine output decrease, abdominal pain, chest pain, fever, chillness or cough. • He almost drinks every day. He often fogets to eat due to drunk. He drank 公賣局米酒 on 11/03 night.
Past History • He denied significant systemic diseases, such as diabetes mellutis , hypertension, heart, kidney, or lung diseases. • Current medicine: nil
Personal History • Allergy: no known allergy • Alcohol: he drinks 米酒 at least 1 bottle per day; betel-nut: denied; cigarette: 1 ppd/day since young age • Over-the-counter medication or chinese herb: denied
Family History • No family history of diabetes mellutis, malignancy, heart, liver, kidney, or hereditary diseases.
Physical Examination • Vital signs: T:36’C , P:116 bpm, R:17/min , BP:137/92 mmhg • General apperance: chronic ill looking • Consciousness: clear, GCS: E4V5M6 • HEENT: conjunctive: not pale, sclera: anicteric pupil: 3mm/3mm , light reflex: +/+, EOM: full/full • Chest: symmetric expansion , clear breathing sound • Heart: regular heart beat without murmur • Abdomen: soft and flat, normoactive bowel, no tenderness liver/spleen: impalpable, no palpable bladder • Extremity: free movement, no pitting edema • Digital rectal exam: yellowishy stool
11/04 Laboratory data • Osmo gap: • Serum Osm – calculated Osm ( 2 [Na] + [BUN]/2.8 + [glucose]/18 + [EtOH]/4.6) = 21.86 mOsm/kg => Anion gap: ?
11/04 Brain CT • Impression: subtle low attenuation in cerebellum and prominent cerebellar sulci. DDX: cerebral cortical atrophy or infarct, pleased clinical correlation.
Impression • Metabolic acidosis with high osmolar gap, etiology? favor methanol intoxication related • Bloody stool, favor hemorrhoid related
Plans • Closely monitor vital signs, mental status and consult ophthalmologist for thorough visual exam • Complete metabolic acidosis survey, please check anion gap, ketone, lactate, ethyl alcohol and urine AG • Suggest the patient take ethanol as antidote • Arrange hemodialysis for increasing methanol elimination • Follow up methanol level, blood Osm, and ABG • Give thiamine and watch out for alcohol withdrawal
Laboratory data HD HD
Other examination • 11/07 Sigmoidoscopy : Impression: No active bleeder. Colon polyp, R-S colon Mixed hemorrhoid. • 11/09 Brain MRI : Impression: Normal brain MR study.
11/09 Follow-up Ocular Examination • s/s : still blurred vision (ou) • VA: ou CF/50cm • RAPD: + (od) • clear corea, AC and lens (ou) • fundus: decreased hyperemia of the r’t disc, but disc margin is sl. blurred => Discharge and OPD follow-up !!
Summary of exposure • Methanol are frequently found in high concentration in automotive antifreeze and de-icing solutions, windshield wiper fluid, solvent cleaners, fuels, other industrial products, and adulterant in homemade distillates. • Most serious poisonings occur following ingestion; inhalation and dermal exposures rarely cause toxicity. • Lethal dose – 1 g/kg Toxicity dose – 0.25ml/kg of 100% methanol (>8g) Threshold of treatment – 20~25mg/dL
Methanol metabolism Toxicity Elimination Half life Kidney:3~5% Lung:12% 8 hr 51hr 1 ( Liver ) 33 ( Liver ) 6 20 hr Adult: 8.5 mg/dl/hr Child: 0.88 mg/dl/hr @
Clinical features • Early toxicity(acute intoxication) CNS:sedation, disinhibition, ataxia, headache GI:abdominal pain, nausea, vomiting
Clinical features • Late toxicity(severe metabolic acidosis develops 6-12 hours after exposure ) HEENT:Ocular toxicity CV: tachycardia, arrythmia, bradycardia (fatal poisoning), cardiac arrest, severe hypotension Respiratroy: tachypnea, sudden respiratory failure Neurologic: coma, seizure, basal ganglia necrosis with parkinsonian features, polyneuropathy, optic atrophy GI: abdominal pain, anorexia, nausea, vomiting, necortizing pancreatitis (severe poisoning)
Clinical features GU: acute renal failure, hamaturia Acid-base: metabolic acidosis (concurrent ethanol ingestion may delay acidosis > 1 hr ) Electrolyte: hypomagnesemia, hypokalemia, hypophophatemia Musculoskeletal: rhabdomyolysis (severe poisoning) Reproductive: birth defects of CNS (ingested together with other solvents) Keypoints of PE: Vital sign, mental status, pupuils, thorough visual exam
Normal Relative afferent pupillary defect @
Diagnostic testing • Finger sugar (rule out hypoglycemia, DKA, HHNK) • Arterial or venous blood gas , renal function, electrolytes, serum osmolality, methanol, ethanol , ethylene glycol, isopropanol concentration, lactate, acetaminophen and salicylate levels (to help determine diagnosis) high anion gap? HCO3 <8 ? Osm gap > 10 ? mild elevated lactate levels? • ECG • Pregnancy test in women of childbearing age
Treatment • Keep airway, breathing, circulation: * Endotracheal intubation if mental status change or respiratory failure hyperventilated with large minute ventilations to prevent profound acidemia * IV crystalloid + vasopressors if hypotension
Treatment • Decontamination : * GI – not very useful ( methanol is rapidly absorbed and binds poorly to activated charcoal). Gastric aspiration by NG tube within 60 mins of ingestion maybe useful. * Eye – irrigate with water for > 15 mins * Dermal – remove contaminated clothing and wash exposed area with soap and water
Treatment • Medication : a. If PH < 7.3, give Sodium bicarbonate 1-2meq/kg bolus + 132 meq in 1L D5W run 150-250cc/hr b. Antidote – ADH inhibition (give as soon as possible) * Fomepizole – 15mg/kg iv loading + 10mg/kg q12h x 4 doses Followed by 15mg/kg q12h if necessary * Ethanol – 8ml/kg of a 10% ethanol solution ivf loading + 1ml/kg/hr of 10% ethanol solution. Titrate serum EtOH to 100 mg/dL or
Treatment • Hemodialysis -- rapidly remove both methanol and its toxic acid metabolites (methanol half life 8 hrs 2.5 hrs) * Indication : a. Known methanol intoxication -- High anion gap metabolic acidosis -- End organ damage (visual changes) b. Suspected methanol intoxication -- Unexplained high anion gap metabolic acidosis + high plasma osmolar gap ( PH < 7.3 if strongly suspected, PH < 7.1 if weakly susected)
Treatment • Cofactor therapy – combine with ADH inhibition Folinic acid (leucovorin) 50mg iv q4-6h or Folic acid 50mg IV q4-6h increases clearance of formate • Admission criteria: acidosis, visual symptoms, or methanol > 25mg/dL