Download
1 / 48
480 likes | 623 Vues
This case presentation discusses the admission of a 69-year-old male who ingested approximately 350 ml of an organophosphate compound (陶斯松) in a suicide attempt. Following ingestion on July 12, the patient exhibited symptoms including vomiting, wheezing, and loss of consciousness. He underwent gastric lavage and received treatment including PAM for detoxification. The case highlights the mechanisms of organophosphate toxicity, symptoms of cholinergic crisis, and the clinical approach to management in a critical care setting.

E N D
Toxicology conference 2011.08.12 指導醫師:許景瑋醫師 報告者:fellow 1 陳筱惠
Patient Profile • Name: 林o順 • Sex: male • Age: 69years old • Chart number: 2021918 • Date of admission: 2011/07/12
Chief Complaint • Ingestion of 陶斯松 about 350ml in the morning
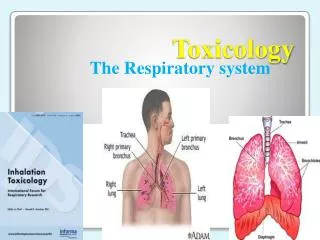
Present Illness • 69 year old man without significant systemic diseases • Ingestion of 陶斯松 about 350ml for suicide attempt on 7/12 morning • He vomited several times just after taking the agent. • At 恩主公 hospital: NG gastric lavage with charchoal • At ER: • Clear consiousness • Associated symptoms?? wheezing, dyspnea, seizure, lacrimation, sweating, diarrhea, abdominal pain, urine incontinence, muscle weakness • He was admitted to MICU-2.
Past History • He denied significant systemic diseases, such as diabetes mellutis , hypertension, heart, kidney, or lung diseases. • Operation history: for bilateral inguinal hernia years ago • Current medicine: nil
Personal History • Allergy: no known allergy • Alcohol: denied; betel-nut: denied; cigarette: 1 ppd/day since young age • Over-the-counter medication or chinese herb: denied
Family History • No family history of diabetes mellutis, malignancy, heart, liver, kidney, or hereditary diseases
Physical Examination • Vital signs: blood pressure: 186/106mmHg; temperature: 35.8’C; pulse rate: 104/min; respiratory rate: 22/min • General apperance: acute ill looking • Eye: pupil 3/3, conjunctiva: not pale, sclera: no icteric • Neck: supple, no lymphadenopathy or jugular vein engorgement • Chest: symmetric expansion breathing sound: bilateral clear, no wheezing or crackles heart sound: regular heart beats, no S3 or S4, no murmurs • Abdomen: soft, not distended, no tenderness liver/spleen: impalpable bowel sound: normoactive • Extremities: no muscle weakness or lower limb pitting edema • Skin: intact, no rash
Impression • Organophosphate intoxication due to suicide attempt • Bilateral inguinal hernia post operation years ago
Plans • Give PAM for antidote (no Atropine??) • O2 support and IVF hydration • Closely monitor vital signs, clinical condition, and respiratory pattern • Check and rollow up plasma cholinesterase level regularly
Intubation Atropine 2pc -> 4pc st for bronchorrhea/dyspnea PAM Cefuroxime Clindamycin Hospitalization course
Cefuroxime Ceftazidime Clindamycin Extubation failure PAM
Extubation Transfer to Nephro ward PAM Ceftazidime
Atropine 1pc q12h Ceftazidime
Atropine 1pc q12h Ceftazidime
Mechanism of action • Organophosphorous compounds bind to acetylcholinesterase (AChE) and render this enzyme non-functional • AChE: the enzyme responsible for hydrolysis of acetylcholine to choline and acetic acid • After period of time, the acetlycholinesterase-organophosphorous compound undergoes "aging," which renders the enzyme irreversibly resistant to reactivation by an antidotal oxime.
Carbamate compounds: transient cholinesterase inhibitors, which spontaneously hydrolyze from the cholinesterase enzymatic site within 48 hours • Carbamate toxicity tends to be of shorter duration than that caused by equivalent doses of organophosphates, although the mortality rates associated with exposure to these chemical classes are similar.
Clinical features • Onset and duration of AChE inhibition varies depending on • Rate of AChE inhibition • Route of absorption • Oral or respiratory exposures: within 3 hours • Dermal absorption: 12 hours • Enzymatic conversion to active metabolites • Lipophilicity • Lipophilic agents are associated with delayed onset of symptoms (up to 5 days) and prolonged illness (greater than 30 days).
Acute toxicity • Cholinergic excess: autonomic nervous system, neuromuscular junction, and central nervous system (CNS)
SLUDGE/BBB : Salivation, Lacrimation, Urination, Defecation, Gastric Emesis, Bronchorrhea, Bronchospasm, Bradycardia • DUMBELS: Defecation, Urination, Miosis, Bronchorrhea/Bronchospasm/Bradycardia, Emesis, Lacrimation, Salivation
Intermediate syndrome • 10~40%, 24~96hours • Characteristic neurological findings: neckflexion weakness, decreased deep tendon reflexes, cranial nerve abnormalities, proximal muscle weakness, and respiratory insufficiency • Risk factors: • Highly fat-soluble organophosphorous agent(大滅松、芬殺松、亞素靈) • Inadequate doses of oximes
Delayed neurotoxicity • 1~3 weeks • 達馬松、三氯松、美文松、陶斯松、巴拉松 • Inhibition of neuropathy target esterase (NTE) • S/S: • Transient, painful "stocking-glove" paresthesias a symmetrical motor polyneuropathy (flaccid weakness of lower extremities, then ascends to upper extremities, primarily distal muscle) • Sensory disturbances: mild
EMG/NCV: decreased firing of motor conduction units • Histopathologic sections of peripheral nerves: Wallerian (or "dying-back") degeneration of large distal axons
Diagnosis • Clinical features of cholinergic excess • Petroleum or garlic-like odor • Dimethyl or a diethyl compound?? • Dimethyl compounds undergo rapid aging, making early initiation of oxime therapy critical. • Diethyl compounds may exhibit delayed toxicity, and may require prolonged treatment.
A trial of 1 mg atropine in adults (or 0.01 to 0.02 mg/kg in children) • The absence of signs or symptoms of anticholinergic effects following atropine challenge strongly supports the diagnosis of poisoning with an acetylcholinesterase inhibitor.
Laboratory abnormalities : • RBC acetylcholinesterase (RBC AChE): Most hospital laboratories are unable to perform this test. • The degree of toxicity • The effectiveness of oxime therapy in regeneration of the enzyme • Chronic or occupational exposure • Plasma (or pseudo-) cholinesterase
Management • Early intubation: • CNS respiratory center depression • Nicotinic receptor mediated diaphragmatic weakness, bronchospasm, and copious secretions • Avoid the use of succinylcholine when performing rapid sequence intubation (RSI) in patients with organophosphate (OP) poisoning • Succinylcholine is metabolized by acetylcholinesterase.
Adequate volume resuscitation with isotonic crystalloid (eg, normal saline or lactated Ringer's solution)
Decontamination: topical exposure • We generally do not perform gastric lavage. • Substantial risk of aspiration in patients with increased secretions and decreased mental status • Not decrease morbidity or mortality • Patients presenting within 1 hour of an organophosphorous agent or carbamate ingestion: activated charcoal 1 g/kg (max dose 50 g)
Forced emesis is contraindicated because of the risk of aspiration and seizures. • Urinary alkalinization has been suggested, but there is no clear evidence that this intervention improves outcome.
Atropine: • Compete with acetylcholine at muscarinic receptors; ineffective in treating neuromuscular dysfunction (nicotinic receptors) • A dose of 2 to 5 mg IV for adults and 0.05 mg/kg IV for children no effect, then bouble dose every 3~5 mins until pulmonary muscarinic S/S alleviating (clearing of respiratory secretions, cessation of bronchoconstriction) infusion of 10~20% of loading dose/hour • Atropine overdose
Concurrent use of atropine to prevent worsening symptoms due to transient oxime-induced acetylcholinesterase inhibition • Dose:
Benzodiazepines: • Organophosphorous agent-induced seizures • Prophylactic use has been shown to decrease neurocognitive dysfunction after organophosphorous agent poisoning.
7/13 blood culture: negative • 7/13 urine culture: negative • 7/15 sputum culture: Ps.aeruginosa + Kleb.pneumoniae