Download
1 / 69
700 likes | 962 Vues
PATHOLOGY OF HYPOTHALAMIC-PITUITARY AREAS. Department of Internal Medicine №2 as.-prof. Martynyuk L.P. Plan of lecture. Anatomy and physiology of hypothalamus and pituitary gland. Classification of hypothalamus and pituitary gland. Etiology of hypothalamo – pituitary disorders.

E N D
PATHOLOGY OF HYPOTHALAMIC-PITUITARY AREAS Department of Internal Medicine №2 as.-prof. Martynyuk L.P.
Plan of lecture • Anatomy and physiology of hypothalamus and pituitary gland. • Classification of hypothalamus and pituitary gland. • Etiology of hypothalamo – pituitary disorders. • Acromegaly, giantism: diagnostic criteria and treatment • Pituitary dwarfism: diagnostic criteria and treament. • Hypopituitarism: diagnostic criteria and treatment. • Diabetes insipidus: diagnostic criteria and treatment. • Inapropritiative secretion of vasopresin: diagnostic criteria and treatment.
Plan of lecture • Epidemiology of obesity. • Health consequences. • Etiology of obesity. • Predisposing factors of obesity. • Classification of obesity. • Clinical manifestations of obesity: • Alimentary obesity. • Hypothalamic obesity. • Pickwickian syndrome. • Barrakcer – Simmons’s disease (progressing lipodystrophia). • Dercum’s disease (generalized painful lipomatosis.) • Babinsky-Frelych’s disease (adipose-genital dystrophy). • Lorens – Moon – Bydlya’s syndrome. • Morganyi – Stuart – Morel’s syndrome. • Postnatal neuroendocrine syndrome. 15. Treatment of obesity.
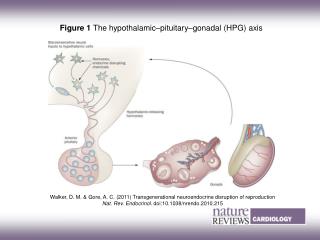
The pituitary gland is the “master gland”, which lies in a bony structure, the sella turcica, located at the base of the skull. The gland is a small organ about I cm long; it weighs 500 mg and is divided into two parts, anterior (adenohypophysis) and posterior (neurohypophysis). The anterior pituitary secretes • corticotropin (ACTH) • Prolactin • Somatotropin (growth hormone (GH) • gonadotropins [follicle-stimulating (FSH) and luteinizing (LH) hormones] • thyrotropin (TSH) • melanocyte-stimulating hormones (MSH). In the nerve endings of the posterior pituitaryare stored • Vasopressin (antidiuretic hormone, ADH) • Oxytocin
The hypothalamusplays an important role in hormone regulation by secreting a series of small peptides which stimulate or inhibit the synthesis and release of hormones by the anterior pituitary • First hypothalamic releasing hormone identified in 1970 was TRH by Schalli and Guilemin who von Nobel prize in medicine for their discoveries in1977 • Realising Inhibiting • CRG • TRG • LGRG • FSRG • GRH - GIH (somatostatin) • PRG - PIF (dopamine) • MRG - MIH
Regulation • FEEDBACK: Hormone secretion → delivery to target cells → hormone recognition by receptors in target cells → biologic effect → hormone degradation → signal from target cells to stop further hormonesecretion
Etiology of hypothalamo – pituitary disorders 1.Trauma 2. Infectious diseases: • acute (scarlet fever, influenza) • chronic (tuberculosis, malaria, toxoplasmosis) 3. Tumor or metastasis 4. Vascular damaging (thrombosis, thromboembolia) 5. Metabolic disorders (xanthomathosis) 6. Congenital pituitary hypo – or aplasia (syndrome of “empty sella turcica” 7. Genetic predisposition 8. Idiopathic
Classificationof hypothalamo – pituitary disorders • Adenohypophysis disorders 1. Secretion of GH • overproduction: acromegaly, giantism • dificiency: pituitary dwarfism 2. Secretion of ACTH • overproduction: Cushing’s syndrome, hypothalamic syndrome 3. Secretion of Prolactin • overproduction: hyperprolactinemia, galactorhea-amenorhea 4. Secretion of TSH 5. Secretion of Gonadotropines: adiposogenital-dystrophy 6. Hypothalamic obesity • Neurohypophysis disorders 1. Deficiency of vasopressin: diabetes insipidus 2. Inapropritiative secretion of vasopressin
GROWTH-HORMONE EXCESS(acromegaly and gigantism) Chronic, debilitating disorder resulting from exessive secretion of GH and resulting in production of insulin-like growth factor 1 (IGF-1), which lead to typical picture: gigantismbefore puberty and to acromegaly after puberty.
Pharmacologic therapy • A dopaminergic agonist and ergot derivative, 2a-bromergocriptine (bromocriptinef 10 to 60 mg/day, (clinical remissions in 73 % patients, normalization of GH level in 22 % of patients). Side effects include nausea, orthostatic hypotension, constipation, digital vasospasm, and peptic ulcer. 2. Comatostatin analogues: octreotide, sandostatin (clinical remissions in 90 % patients, normalization of GH level in 50 % of patients). Side effects include nausea, diarrhea, gallstones, glucose intolorence.
Treatment Surgery: - Transsphenoidal hypophysectomy is the procedure of choice. Advantages: effectivity in nearly 90 % of the patients, simplicity and low morbidity. Side effects: hypupituitarism, diabetes insipidus, recurrence of symptoms. • Craniotomy is reserved for large tumors with suprasellar extension and involvement of the optic chiasm. • Cryohypophysectomy (destruction of the pituitary by cold injury) can reduce the secretion of GH (without causing hypopituitarism) in 88 % of the patients. External irradiation: • External beam • Gamma knife
PITUITARY DWARFISM (GROWTH FAILURE) - it is the disease caused by decreased secretion of GH by pituiatary gland or decreased sensitivity of peripheral tissues to this hormone and leads to growth retardation.
Treatment. • Balanced diet. • Complex of physical exercises. • Pharmacotherapy. • GH (synthetic). • Anabolic steroids under the control of biologic (osteal) age. • Thyroid replacement. • Replacement with gonodal steroids is never indicated until puberty normally occurs. These agents in high doses can hasten bone maturation and epiphyseal closure, thereby limiting the height which may ultimately be reached. • Vitamintherapy. • Surgical therapy (a craniopharyngioma presents special therapeutic problems, usually necessitating removal of tumor tissue or drainage of fluid from tumor cysts.
HYPOPITUITARISM It is the syndrome, which is characterized by deficiency of one or more anterior pituitary hormones.
Treatment - eliminating the underlying cause - replacing the deficient hormones • Pituitary tumors should be removed surgically, although irradiation and drug therapy (bromocriptine) are also available. • Treatment of acute and chronic infection Hypothalamic peptides or pituitary hormones are not suitable for hormone replacement : (1) The human hormones are difficult to oblain in pure form; (2) because of their nature and short halh-life they have to be given parenterally and frequently; (3) since they stimulate antibody formation, their activity is lost a few weeks after initiation of therapy. Under these circumstances the usual practice is to administer the hormones produced by the target glands.They are available in pure form and are relatively inexpensive.
Replacement therapy • Hydrocortisone 20 - 30 mg/day, prednisolone 5 - 15 mg/day • Replacement with gonodal steroids is never indicated until puberty normally occurs. These agents in high doses can fasten bone maturation and epiphyseal closure, thereby limiting the height which may ultimately be reached. • In males testosterone therapy is recommended. • Premenupausal females with ovarian failure should be treated with estrogens. • Thyroid drugs (L-thyroxin, euthyrox) • Vitamines, anabolic hormones
DIABETES INSIPIDUS is a clinical disorder characterized by the excretion of large quantities of diluted urine and caused either by failure of ADH release (hypothalamic diabetes insipidus) or by lack of response of the tubules to normal quantities of circulating ADH (nephrogenic diabetes insipidus).
Treatment • Etiologic • Pathogenetic • Hypothalamic DI • Adiurecrin powder nasal spray0,03 g 1 – 3 times a day • Adiuretin in drops 1 – 3 times a day • Synthetic lysine vasopressin, desmopressin 1 to 2 sprays three or four times a day. • Pituitrin 0,5 – 1 ml subcutaneous 2 – 3 times a day. • Nephrogenic DI • chlorpropamide 100 to 500 mg/day • Tegretol (400 mg/day) • diuretics (thiazide diuretic (50 to 100 mg/day of hydrochlorothiazide) is added to enhance the sodium depletion and impair the ability of the tubules to generate a dilute urine)
THE SYNDROME OF INAPPROPRIATE SECRETION OF ADH is characterized by persistent ADH secretion and the excretion of a concentrated urine despite serum hypoosmolality.
Treatment • Identification of the underlying cause and measures to correct it are important therapeutic goals. • The mainstay of therapy for the syndrome of inappropriate ADH secretion is water restriction to less than 1 L/day. Weight loss and an increase in serum sodium concentration will occur 3 to 7 days after therapy has been started. • In patients who present with marked hyponatremia (less than 110 meq/L) and neurologic symptoms, particularly seizures, infusion of 250 ml of hypertonic saline (3 % NaCI) over 2 to 4 h is indicated. • Furosemide in combination with intravenous or oral sodium chloride sometimes is effective. The therapeutic goal is to increase free water clearance and at the same time to replace the sodium urinary losses .
OBESITY is a state of increased body weight, specifically fat, of sufficient magnitude to exert adverse effects on health (Obesity is characterized by excessive accumulation of body fat)
Etiology The cause of obesity is simple – consuming more calories than are expended as energy. Why patients become obese? Why persons consume more calories than they expend?
Epidemiology • Nearly 30 % of world population suffers from different stages of obesity • Its importance lies in the many, often serious, complications to which obese people are subject. In these complications that warrant undertaking a treatment that is so often unsuccessful
Predisposing factors • Sex • Endocrine factors. (Certain diseases of endocrine glands are associated with obesity i.e. hypothyroidism, Cushing’s disease, hypogonadism.) • Psychological factor • Brain (especially, hypothalamic injury)
Body weight regulation • Enzymes, metabolic defects of peripheral receptors • Imbalance on the hypothalamus level • Endocrine system disorders • Defects of sympathetic regulation
Classification by Egorov • Alimentary • Endocrine • Cerebral (hypothalamic)
Classification due to deposition of fat tissue • upper type (abdominal, android); • lower type (gluteofemoralis, gynoid).
Abdominal obesity • Waist/hip ration - >1,0 in men - > 0.85 in women • Waist circumference - >102 cm in men - > 82 cm in women • Both methods identify those with increased CVD risk
Brock’s index (N: weight = height – 100) I. Weight excess < 30 %. II. Weight excess 30 – 50 %. III. Weight excess 50 – 100 %. IV. Weight excess > 100 %. Kettle’s index BMI (body mass index) (N: weight, kg / height, m2) Overweight: 25,1 – 29,9 I. 30,0 – 34,9 II. 35,0 – 39,9 III. > 40,0 Classification due to stages of obesity
Weight (kg) prominent obesity obesity overweight normal low weight Body mass index Height (sm)