Download
1 / 36
1.42k likes | 8.44k Vues
Contracted Pelvis. Dr.Pooja Rajbhara Senior Resident OBGY. DEFINITION. Anatomically , contracted pelvis is defined as one where the essential diameters of one or more planes are shortened by 0.5 cm.

E N D
Contracted Pelvis Dr.PoojaRajbhara Senior Resident OBGY
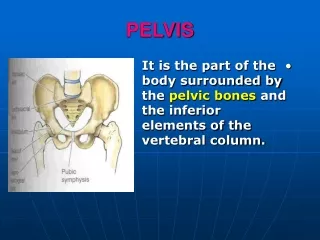
DEFINITION • Anatomically, contracted pelvis is defined as one where the essential diameters of one or more planes are shortened by 0.5 cm. • But of more importance is the obstetric definition which states that alteration in the size and/or shape of the pelvis of sufficient degree so as to alter the normal mechanism of labour in an average size baby.
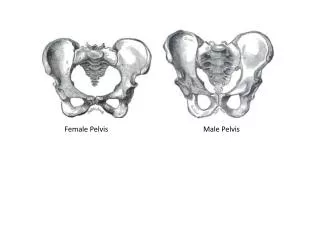
VARIATIONS OF FEMALE PELVIS However, on the basis of the shape of the inlet, the female pelvis is divided into four parent types. • Gynecoid (50%) • Anthropoid (25%) • Android (20%) • Platypelloid(5%)
There may be 14 types of parent pelvis either in pure form or in combination.
ETIOLOGY OF CONTRACTED PELVIS Common causes of contracted pelvis are: (1) Nutritional and environmental defects — • Minor variation: common • Major: Rachitic and osteomalacic — rare (2) Diseases or injuries affecting the bones of the pelvis — fracture, tumours, tubercular arthritis; • Spine — Kyphosis, scoliosis, spondylolisthesis, coccygeal deformity; • Lower limbs — Poliomyelitis, hip joint disease. (3) Development defects — Naegele’s pelvis, Robert’s pelvis; High or low assimilation pelvis.
MECHANISM OF LABOR IN CONTRACTED PELVIS WITH VERTEX PRESENTATION • FLAT PELVIS -In the flat pelvis, the head finds difficulty in negotiating the brim and once it passes through the brim, there is no difficulty in the cavity or outlet. The head negotiates the brim by the following mechanism: • The head engages with the sagittal suture in the transverse diameter. • Head remains deflexed and engagement is delayed. • If the anteroposterior diameter is too short, the occiput is mobilized to the same side, to occupy the sacral bay. The biparietal diameter is thus placed in the sacro-cotyloid diameter (9.5 cm or 8.5 cm) and the narrow bitemporal diameter is placed in the narrow conjugate. If lateral mobilization is not possible, there is a chance of extension of the head leading to brow or face presentation.
Engagement occurs by exaggerated parietal presentation so that the super-subparietal diameter (8.5 cm), instead of the biparietal diameter (9.5 cm), passes through the pelvic brim. • Mouldingmay be extreme and often there is an indentation or even a fracture of one parietal bone. However, the caput that forms is not big. • Once the head negotiates the brim, there is no difficulty in the cavity and outlet and normal mechanism follows. • GENERALLY CONTRACTED PELVIS: In this type of pelvis, the shape remains unaltered but all the diameters in the different planes — inlet, cavity and outlet are shortened. There is difficulty from the beginning to the end.
DIAGNOSIS OF CONTRACTED PELVIS • Past History: 1.Medical 2.Obstetric • Physical Examination: stature, stigma • Abdominal Examination: • Inspection: Pendulous abdomen specially in primigravidae, is suspicious of inlet contraction. Obstetrical: In primigravidae, usually there is engagement of the head before the onset of labor. Presenceof malpresentation in primigravidae, gives rise to a suspicion of pelvic contraction. • Assessment of the pelvis (pelvimetry): Assessment of the pelvis can be done by bimanual examination: clinical pelvimetry or by imaging studies — Radio-pelvimetry, Computed Tomography (CT) and Magnetic Resonance Imaging (MRI).
Clinical pelvimetry: This is done manually. • Time: In vertex presentation, the assessment is done at any time beyond 37th week but better at the beginning of labor. Because of softening of the tissues, assessment can be done effectively during this time. • Procedures: The patient is to empty the bladder. The pelvic examination is done with the patient in dorsal position taking aseptic preparations. The following features are to be noted simultaneously: (1) State of the cervix (2) To note the station of the presenting part in relation to ischial spines (3) To test for cephalopelvic disproportion in nonengagedhead and (4) To note the resiliance and elasticity of the perineal muscles. • Steps: The internal examination should be gentle, thorough, methodical and purposeful. It should be emphasized that the sterilized gloved fingers once taken out should not be reintroduced.
Sacrum — The sacrum is smooth, well curved and usually inaccessible beyond lower three pieces. The length, breadth and its curvature from above down and side to side are to be noted. • Sacrosciaticnotch — The notch is sufficiently wide so that two fingers can be easily placed over the sacrospinous ligament covering the notch. The configuration of the notch denotes the capacity of the posterior segment of the pelvis and the side walls of the lower pelvis. • Ischialspines — Spines are usually smooth (everted) and difficult to palpate. They may be prominent and encroach to the cavity thereby diminishing the available space in the mid pelvis. • Ilio-pectineal lines — To note for any beaking suggestive of narrow fore pelvis (android feature). • Sidewalls — Normally they are not easily palpable by the sweeping fingers unless convergent.
Posterior surface of the symphysis pubis — It normally forms a smooth rounded curve. Presence of angulation or beaking suggests abnormality. • Sacrococcygeal joint — Its mobility and presence of hooked coccyx, if any, are noted. • Pubic arch — Normally, the pubic arch is rounded and should accommodate the palmar aspect of two fingers.Configurationof the arch is more important than pubic angle. • Diagonal conjugate — After the procedure, the fingers are now taken out.
Pubic angle: The inferior pubic rami are defined and in female, the angle roughly corresponds to the fully abducted thumb and index fingers. In narrow angle, it roughly corresponds to the fully abducted middle and index fingers. • Transverse diameter of the outlet (TDO) — It is measured by placing the knuckles of the first interphalangeal joints or knuckles of the clinched fist between the ischialtuberosities. • Anteroposterior diameter of the outlet—The distance between the inferior margin of the symphysis pubis and the skin over the sacrococcygeal joint can be measured either with the method employed for diagonal conjugate or by external calipers.
EFFECTS OF CONTRACTED PELVIS ON PREGNANCY AND LABOR • Pregnancy:(1) There is more chance of incarceration of the retroverted gravid uterus in flat pelvis; (2) Abdomen becomes pendulous specially in multigravida with lax abdominal wall; (3) Malpresentations are increased 3–4 times and so also increased frequency of unstable lie. • Labor: (1) There is; increased incidence of early rupture of the membranes; (2) Incidence of cord prolapse is increased; (3) Cervical dilatation is slowed; (4) There is increased tendency of prolonged labor and in neglected cases, obstructed labor with features of exhaustion, dehydration, keto-acidosis and sepsis. (5) There is increased incidence of operative interference, shock, postpartum; and hemorrhage and sepsis. • Maternal injuries: The injuries of the genital tract may occur spontaneously or following operative delivery. There is increased maternal morbidity and mortality. • Fetal hazards: Fetal risks are due to trauma and asphyxia.Thenet effect leads to increased perinatal mortality and morbidity.
DISPROPORTION • Disproportion, in relation to the pelvis is a state where the normal proportion between the size of fetus to the size of the pelvis is disturbed. The disparity in the relation between the head and the pelvis is called cephalopelvic disproportion. • Disproportion may be either due to an average size baby with a small pelvis or due to a big baby with normal size pelvis (hydrocephalus) or due to a combination of both the factors. • Pelvic inlet contraction is considered when the obstetric conjugate is < 10 cm or the greatest transverse diameter is < 12 cm or diagonal conjugate is < 11 cm.
Contracted Midpelvis: Midpelvis is considered contracted when the sum of the inter-ischialspinous and posterior sagittal diameters of the mid pelvis (normal: 10.0 + 5 = 15.0 cm) is 13.0 cm or below. • Contracted outlet is suspected when the inter ischial tuberous diameter is 8 cm or less. A contracted outlet is often associated with midpelvic contraction.
DIAGNOSIS OF CEPHALOPELVIC DISPROPORTION (CPD) AT THE BRIM • Clinical — (a) Abdominal method; (b) Abdominovaginal (Muller-Munro Kerr) • Imaging pelvimetry • Cephalometry— (a) Ultrasound; (b) Magnetic Resonance Imaging; (c) X-ray
Clinical: In multigravida, a previous history of spontaneous delivery of an average size baby, reasonably rules out contracted pelvis. But in a primigravida with nonengagement of the head even at labor, one should rule out disproportion. • Abdominal method: The patient is placed in dorsal position with the thighs slightly flexed and separated. The head is grasped by the left hand. Two fingers (index and middle) of the right hand are placed above the symphysis pubis keeping the inner surface of the fingers in line with the anterior surface of the symphysis pubis to note the degree of overlapping, if any, when the head is pushed downwards and backwards.
Inferences: • The head can be pushed down in the pelvis without overlapping of the parietal bone on the symphysispubis — no disproportion. • Head can be pushed down a little but there is slight overlapping of the parietal bone evidenced bytouch on the under surface of the fingers (overlapping by 0.5 cm or 1/4” which is the thickness of thesymphysispubis) — moderate disproportion. • Head cannot be pushed down and instead the parietal bone overhangs the symphysis pubis displacingthe fingers — severe disproportion. • The abdominal method can be used as a screening procedure. At times, it is difficult to elicit due to deflexed head, thick abdominal wall,irritableuterus and high floating head.
Abdominovaginal method (Muller-Munro Kerr): • This bimanual method is superior to the abdominal method as the pelvic assessment can be done simultaneously. Muller introduced the method by placing the vaginal finger tips at the level of ischial spines to note the descent of the head. Munro Kerr added placement of the thumb over the symphysis pubis to note the degree of overlapping. • Bowel bladder preparation. • Lithotomy position.
Inferences: (1) The head can be pushed down up to the level of ischial spines and there is no overlapping of the parietal bone over the symphysis pubis — no disproportion; (2) The head can be pushed down a little but not up to the level of ischial spines and there is slight overlapping of the parietal bone — slight or moderate disproportion; and (3) The head cannot be pushed down and instead the parietal bone overhangs the symphysis pubis displacing the thumb — severe disproportion. • Limitations of clinical assessment: (1) The method is only applicable to note the presence or absence of disproportion at the brim and not at all applicable to elicit midpelvic or outlet contraction (2) The fetal head can be used as a pelvimeter to elicit only the contraction in the anteroposterior plane of the inlet; but when the contraction affects the transverse diameter of the inlet, it is of less use.
X-ray pelvimetry: Lateral X-ray view with the patient in standing position is helpful in assessing cephalo- pelvic proportion in all planes of the pelvis — inlet, midpelvic and outlet. • Cephalometry: While a rough estimation of the size of the head can be assessed clinically, accurate measurement of the biparietal diameter would have been ideal to elicit its relation with the diameters of the planes of a given pelvis through which it has to pass. In this respect ultrasonographic measurement of the biparietal diameter or Magnetic Resonance Imaging (MRI) gives superior information. The average biparietal diameter measures 9.4–9.8 cm at term. • Magnetic Resonance Imaging (MRI): MRI is useful to assess the pelvic capacity at different planes. It is equally informative to assess the fetal size, fetal head volume and pelvic soft tissues which are also important for successful vaginal delivery (p. 650).
Degree of disproportion and contracted pelvis: Based on the clinical and supplemented by imaging pelvimetry, the following degrees of disproportion at the brim are evaluated. (1) Severe disproportion: Where obstetric conjugate is < 7.5 cm (3”). Such type is rare to see. (2) Borderline: Where obstetric conjugate is between 9.5 and 10 cm. When both the anteroposterior diameter (< 10 cm) and the transverse diameter (< 12 cm) of the inlet are reduced, the risk of dystocia is high than when only one diameter is contracted.
MANAGEMENT OF CONTRACTED PELVIS INLET CONTRACTION: • Minor degrees of inlet contraction does not give rise to any problem and the cases are left to have a spontaneous vaginal delivery at term. • The moderate and the severe degrees are to be dealt by any one of the following: • Preterm induction of labor • Elective cesarean section at term • Trial labor
TRIAL LABOR: It is the conduction of spontaneous labor in a moderate degree of cephalo-pelvic disproportion, in an institution under supervision with watchful expectancy, hoping for a vaginal delivery. Contraindications: (1) Associated midpelvic and outlet contraction; (2) Presence of complicating factors like elderly primigravida, malpresentation, postmaturity, post cesarean pregnancy, pre-eclampsia, medical disorders like heart disease, diabetes, tuberculosis, etc. (3) Where facilities for cesarean section is not available round the clock.
Conduction of trial labor: • Spontaneous in onset. • NPO • Partograph • Monitoring • Augmentation of labor
How long the trial to be continued? • Termination of trial labor: • Advantages of trial labor: • Disadvantages of trial labor:
MIDPELVIC AND OUTLET DISPROPORTION • Cephalopelvicdisproportion at the outlet is defined as one where the biparietal-suboccipitobregmatic plane fails to pass through the bispinous and anteroposterior planes of the outlet. • Management: elective Caesarean section, vaginal delivery.
CASES SEEN LATE IN LABOR is not an uncommon problem in the developing countries. The principles of management rest on: (i) Cesarean section to avoid difficult forceps; (ii) Forceps with deep episiotomy; (iii) Symphysiotomyfollowed by ventouse (iv) Craniotomy if the fetus is dead.