Download
1 / 81
810 likes | 1.13k Vues
Measuring Your Department’s Progress in the Advancement of Pharmacy Practice and Patient Safety CSHP Professional Practice Conference - Jan 2006 Patricia Macgregor, Nancy Roberts Editorial Board members. Outline. Overview of the sections of the 2003/04

E N D
Measuring Your Department’s Progress in the Advancement of Pharmacy Practice and Patient SafetyCSHP Professional Practice Conference - Jan 2006Patricia Macgregor, Nancy RobertsEditorial Board members
Outline • Overview of the sections of the 2003/04 Hospital Pharmacy in Canada Report (HPCR) • Using ave. results for all hospital types • Specialty Focus of the 2003/04 Report • HPCR 2003/04 Indicators and trends • Conducting a Self-Operational Review • Using specific results by hospital size & type • Aligning Your Organizations Priorities • Testimonials
Hospital Pharmacy in Canada Report (HPCR) • Measuring hospital pharmacy progress • Data collection every two years • Also known as “Lilly” report • www.lillyhospitalsurvey.ca
HPCR Sections • Demographics • Clinical Pharmacy Services • Drug Information and Drug Use Evaluation • Drug Distribution • Drug Purchasing and Inventory Control • Human Resources • Medication Safety
HPCR Sections continued • Technology • Education and Research • Pharmacy Staffing and Drug Costs for Clinical Programs - Acute Care Hospitals - Pediatric Hospitals • Benchmarking
2003/04 HPCR Report Focus • Medication safety and role of pharmacy leaders • Clinical practice, direct patient care, pharmacist prescribing • Incident reporting and reduction strategies • Distribution delivery systems • Escalating drug costs - utilization issues • Human resources – impacts of shortages • Technology applications
Demographics • 144 hospitals responded Nationally • Inclusion criteria – 100 beds total, 50 acute beds • 77% response rate overall • 59% of respondents were multi-site facilities, similar to previous survey (higher in BC, Prairies and Atlantic)
Clinical Data Captured • Staffing allocations per specialty program • Clinical pharmacy activity by type with occurrence rate • Specific clinical activity priority and service level • Methods and types of practice evaluation • Prescribing privileges by profession • Pharmacist prescribing authority by activity • Clinical practice models and seamless care
Clinical Practice Trends • Decentralizing pharmacists may decrease medication errors by 45%.* • Centralized pharmacist -errors/bed 3.15 • Centralized with occasional unit visits -errors/bed 1.93 • Decentralized pharmacist -errors/bed 1.74 • % clinical time unchanged, at 38%, from previous surveys *(Bond et al. Pharmacotherapy 2002 22 (2):134-47)
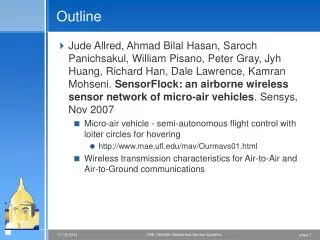
Figure F-2. Proportion of Time Spent by Pharmacists in Each Category 2003/04
Outpatient Pharmacist FTE Ratios Average 0.14 FTE pharmacist/10,000 visits • DVT/anticoagulation 2.02 FTE/10,000 visit • Infectious disease 2.00 FTE • Cardiovascular/lipid 1.67 FTE • Diabetes 1.16 FTE • Hematology/oncology 1.06 FTE • Emerg 0.02 FTE
Inpatient Pharmacist FTE Ratios Average 0.53 FTE pharmacist/10,000 pt days • Adult intensive care 1.53 FTE/10,000day • Adult medicine 0.65 FTE • Adult rehabilitation 0.55 FTE • Adult surgical 0.51 FTE • Adult mental health 0.47 FTE • Geriatrics 0.36 FTE • Pediatric medical 1.27 FTE
Clinical Activities Documentation • # interventions per admission – 0.64 • Increase from 0.6 in 2001/02 and 0.53 in 1999/00 • Annual interventions per pharm FTE – 645 • Still 20% respondents who do document do not do it in the patient chart • Pharmacokinetic documentations on the increase
Priority Ranking vs Actual Activity • Bond et al – 6 clinical services associated with lower total cost of care • DUE, drug information, ADE monitoring, Drug protocol management, medical rounds participation, admission drug histories • Yet none was reported by more than 70% of respondents as being among the top 10 priorities • Participants rated clinical services by priority and by extent offered – striking discrepancy
Clinical Practice Models and Evaluation • 81% reported clinical practice services NOT offered to some inpatients • Equals 33% of inpatient beds • Pharmaceutical care – 70% reported using - average 30 beds serviced • Only 17% evaluate clinical practice
Prescribing Privileges • Pharmacists 66% • Midwives 45% • Nurse practitioners 47% • Other professionals 20%
Pharmacists Prescribing • Lab tests – 21% • Independent dosage adjustments – 23% • New therapy – 5% • Dependent, dosage adjustment – 46% • Dependent, new therapy -13%
Seamless Care-Discharge Information Provided • Medications at discharge 95% • Medications discontinued 68% • Care Plan 56% • Monitoring Values 59% • Diagnosis 46%
Drug Information and DUE • DUE • 0.8 FTE pharmacist • 0.5FTE support staff • Drug Information - 1.3 FTE pharmacists - 0.4 FTE support staff
Drug Distribution and Delivery • Systems used • Order entry • Order verification • MARs, medication profiles etc • Technician check technician • IV admixture • Oncology • Ambulatory services
Distribution Delivery Systems • Traditional delivery some beds 63% • Total wardstock 21% • Unit dose, >90% beds 31%
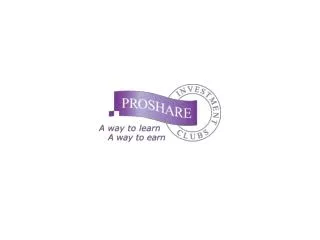
Figure D-2. Proportion of Beds Serviced by Drug Distribution System 2003/04
Order Entry • Pharmacists 79% • Technicians 78% • Nurses 5% • Physicians 3% • Pharmacist verify pharmacist OE -41% *Significant increase from 01/02 report - 27%
Medication Administration Records (MARs) • Electronic, on-line documentation 10% • Manual 44% • Computer generated 56% • Allergy status on MAR 56% • Cards, tickets (Ontario 4%) 25%
Figure D-4. Technician Activities Checked by other Technicians 2003/04
Drug Purchasing and Inventory Control • PMRB reported sales from drugs increased 14.5% in 2003 • Since 2001/02 report: • Acute care inpatient drug cost/pt day only increased 26 cents. (Ave $31.25) • Emerg costs/patient day increased 24% • Ave inventory increased by 10.6% • CIHI - Drugs = 16.2% of total healthcare costs
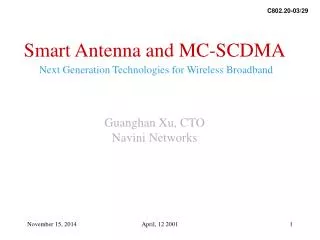
Figure E-1. Percentage of Drug Expenses by Patient Care Area 2003/04
Human Resources • Paid hours per acute patient day, average unchanged at 0.74 • Staffing Ratios • Pharmacist 40% • Technician 46% • Support staff 7% • Management 5% • Residents 2%
Human Resource Shortages • 63% of respondents reported vacancies as follows: • Pharmacist vacancies 12.9% • Management 6.9% • Technicians 0.9% • Residency vacancies 13.8% *Concern expressed re reduced student applications
Impact of Human Resource shortages on Patient Care • 67% respondents reduced services overall • 85% reduced direct patient care • 56% reduced implementation of approved service • 52% reduced teaching • 38% reduced hours • 15% reduced distribution
Medication Incident Reporting and Reduction Strategies • 100% use med incident reporting tool • 67% implemented strategies to increase reporting • 63% disclosure policy • 80% have committee to review med safety DTC, risk, quality, MAC, Pharm/nursing • 51% completed self assessment tool • 95% of assessment tools used were ISMP
Medication Safety • Verbal and telephone orders limited 76% • Med orders conditional until pharmacist review 52% • List of non-acceptable abbreviations 40% • High alert medication list identified 38% • Conc. electrolytes removed from patient care areas 72% • Conc. narcotics removed from patient care areas 47% • Standardized heparin concs. 81%
Issues for Patient Safety • Medication safety is related to the extent of pharmacist involvement in direct patient care, yet why is: • Time spent in clinical activity unchanged since 1999 (38%) • Clinical services still NOT provided to some inpatients (33% inpatient beds) • Specific safety initiatives only partially implemented • ? Related to pharmacist shortage
Technology • Pharmacy systems with clinical decision support 40% • Automated max. dosage alerts 28% • Fully interfaced lab results 25% • CPOE 5% • Handheld devices 49% • Wireless network with handheld 8%
Bar Code Technology • FDA - USA mandate bar codes at bedside – by May 2006 • 22% respondents use bar code technology • Up from 11% in 2002
Education and Research • Education - Student training remained a high priority with: • 83% reporting training for under-graduate pharmacy students • 26% reporting training for pharmacy residents • Research • Sites conducting research decreased to 35% from 43% in 1999/2000 ( may be related to the 13.8% residency position vacancy rate)
Hospital Pharmacy in Canada Annual ReportAnalysis of Indicators
Lilly Report User Customizable Benchmarking Report • Paid hours per acute patient day • Paid hours per acute patient day by distribution system • Drug costs per acute patient day • Drug costs per acute admission • Inventory turns • IV production per acute patient day • Interventions per admission
Additional benchmarking tables in the Report • Ave drug costs per day by clinical program • Ave paid hours per admixture – CIVA, oncology, per investigational drug study • Ave paid hours for inventory/procurement and for DUE per $1m drug purchases • Ave paid hours per patient day for high acuity programs e.g bone marrow transplant, neonatal or pediatric ICU • Changes in drug expense by patient care area • Total drug costs by patient care area
What’s Next? How does your Organization shape up in comparison to your peers?
Conducting a Self-Operational Review
Leadership and Management • Bar Code Technology
Leadership and Management • Uses of Bar Code Technology (Numbers too small to break down by site size)