Functional outcomes working group
210 likes | 360 Vues
Functional outcomes working group. Teleconference November 21, 2011. Outline. Hearing Potential measures and endpoints (Plotkin) Final group recommendation Walking Potential measures and endpoints (Schorry) Final Group recommendation Next steps Pulmonary/bladder outcomes (Robertson)

Functional outcomes working group
E N D
Presentation Transcript
Functional outcomes working group Teleconference November 21, 2011
Outline • Hearing • Potential measures and endpoints (Plotkin) • Final group recommendation • Walking • Potential measures and endpoints (Schorry) • Final Group recommendation • Next steps • Pulmonary/bladder outcomes (Robertson) • Jan 12, 2011 meeting
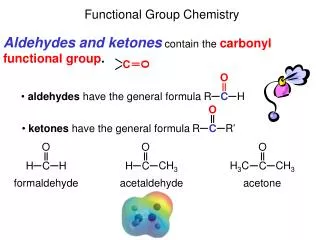
Background: audiograms • Audiogram is standard test of sensitivity • Pure tone average (PTA) • Average of 4 pure tone thresholds • Standardized worldwide • Little variation • Word recognition score (= speech discrimination score) • % correct of monosyllable word list • Not standardized worldwide
“rollover” Maximum Word Recognition = 40% At 80 dBHL PTA = 48.75 dBHL
Background: American Academy of Otolaryngology-Head and Neck Surgery (AAO-HNS) Classification • In these classification systems, a change in one parameter can be masked by stability in the second parameter • Used primarily to describe a study cohort (e.g., Table 1 of manuscript)
Potential measure: maximum word recognition score in clinical trials • WRS disproportionately affected by VS and correlated with QOL • Addressing variability • Recorded word lists • Use of 50-items (rather than 10- or 25-) • Addressing “roll over” • Paradoxical decrease in word recognition score with increasing volume • Need to measure WRS at 2 sound levels • Traditional clinical maximum (level predicted to get best score) • 10-15 dB below • Choose best score of 2 levels
Hearing response criteria:the 95% critical difference threshold Baseline score 95% critical difference threshold Floor effect Ceiling effect Rauch and Halpin, 2005
Proposed Minimal Reporting Standards for Publication of Hearing Results in Clinical Studies • Description of hearing in study ears at baseline (Pure tones x word recognition score Recommend using 3000Hz rather than 4000 Hz for PTAs
Proposed Minimal Reporting Standards for Publication of Hearing Results in Clinical Studies • Description of response to treatment Trial design: Hearing improvement • Established (?) natural history • Primary endpoint • % of patients with hearing response (measured by WRS • Secondary endpoints • % of patients with decrease in PTA (= improvement) of more than 10 dB (response) • Progression-free survival (WRS) at 6, 12, 24 months • Progression-free survival (no decline in PTA) at 6, 12, 24 months
Proposed Minimal Reporting Standards for Publication of Hearing Results in Clinical Studies • Description of response to treatment Trial design: Prevention of hearing loss • No clear natural history for this group • Primary endpoint: • progression-free survival at 6 months (freedom from hearing loss measured by WRS) • Secondary endpoints • PFS at 12 and 24 months (WRS) • PFS at 6, 12, 24 months (PTA) • % of patients with hearing response • % of patients with decrease in PTA (= improvement) of more than 10 dB (response)
Proposed Minimal Reporting Standards for Publication of Hearing Results in Clinical Studies • Encourage investigators to post raw databases as an online supplement
Functional Outcomes Measures Walking Measures
Walking Measures Frequently measured outcome in studies of neurologic disease; rehab studies. Likely appropriate for patients with NF1, NF2, and schwannomatosis with spinal tumors/ gait abnormalities
Timed 10 Meter Walk Time to walk 10 meters (32.8 feet) Measured as time (sec) or velocity (m/sec) Easy to perform; low cost 20% increase or decrease in time is clinically significant change
Use in Other Diseases • Parkinson Disease • Children with neuromuscular diseases • Cerebral palsy, myelomeningocele, etc. • Spinal cord injury • Chronic stroke
Use in other diseases (cont.) • Multiple sclerosis – published use of Timed 25 Foot Walk in trial of Ampyra • Defined responder as one who showed faster walking speed on at least ¾ visits, compared to maximum speed in 5 non-treatment visits • No discernible practice effects in 3 pre-baseline testing sessions over 28 days. • Not previously published in NF
Setting up the 10 meter test • Measure and mark a 10 meter walkway • Add marks at 2 meters and 8 meters. • Patient instructed to walk either at normal comfortable speed, or at fastest speed possible. • Time the walk with a stop watch between 2 meter and 8 meter marks; calculate velocity (meters/sec) • Allows for speed-up and slow-down time at beginning and end of walk • Alternatively, add 2 meters to beginning and end of walk, and measure during the full 10 meters.
Validation of timed 10 meter walk Multiple studies published in multiple sclerosis, rehab literature No practice effect Sensitive to change Valid and clinically useful test to measure improvement in gait for patients with spinal cord injury and multiple sclerosis
Next steps for functional group • Pulmonary outcomes (Jan 2012) • Bowel/bladder outcomes (Jan 2012) • Facial function (March 2012) • Others??