Download
1 / 50
500 likes | 754 Vues
بسم الله الرحمن الرحیم Laser for vascular lesion. دکتر رسول توکلی کیا مرکز تحقیقات پوست و سالک. Vascular birthmarks. Vascular birthmarks, or congenital vascular anomalies, are common lesions that may present in a variety of fashions.

E N D
بسم الله الرحمن الرحیمLaser for vascular lesion دکتر رسول توکلی کیا مرکز تحقیقات پوست و سالک
Vascular birthmarks • Vascular birthmarks, or congenital vascular anomalies, are common lesions that may present in a variety of fashions. • There has traditionally been a significant amount of confusion regarding the nomenclature of these lesions, and the term ‘hemangioma’ has been widely used in the medical literature in reference to a variety of different vascular anomalies.
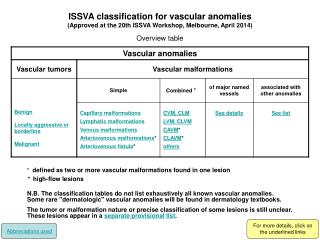
classification system for birthmarks • According to this classification system vascular birthmarks are divided into • Tumors • malformations.
Vascular tumors • Vascular tumors are neoplasms of the vasculature. This category includes • hemangioma of infancy (the most common vascular tumor), • kaposiformhemangioendothelioma, • tufted angioma, • pyogenic granuloma.
Vascular malformations • Vascular malformations represent anomalous bloodvessels without any endothelial proliferation or cellular turnover. In distinction to infantile hemangioma, these lesions tend to be present immediately at birth and persist for a lifetime.
Vascular malformations • Vascular malformations are further classified according to their predominant components, • capillary malformation (port-wine stain, salmon patch) • venous malformation • lymphatic malformation • arteriovenous malformation.
Infantile hemangioma • Infantile hemangioma (hemangioma of infancy) is the most common benign soft tissue tumor of childhood. • It occurs in 1–2%of newborns, and at 1 year of age, 10–12% infants of white skin have one. • Female infants are three times more likely to havehemangiomasthan male infants, and the incidence is increased in premature neonates.
Infantile hemangioma • These lesions vary considerably in their appearance and significance, relating to their size, depth, location, growth pattern, and stage of evolution. • Older descriptive terms for infantile hemangiomas include strawberry, cavernous, and capillary. • These terms are no longer useful and should not be used • Although infantile hemangiomas may occur on any part of the body, they most commonly involve the head and neck regions. • Facial hemangiomas have been noted to have a non-random distribution, with the majority of lesions occurring on the central face at sites of development fusion.
Infantile hemangioma • Hemangiomas may occur as superficial, deep, or mixed lesions. Superficial hemangiomas, when well formed, present as bright red to scarlet, dome-shaped to plaque-like to lobulated papules, plaques, and nodules • They may partially blanch with pressure and are rubbery or non-compressible
Infantile hemangioma • Deep hemangiomas usually present as subcutaneous, partially compressible nodules and tumors, often with an overlying blue hue, prominent venous network, or telangiectasias • These lesions may be warm to palpation. • Combined hemangiomas have both a superficial component and a deep component,n and occur in up to 25–30% of patients. • They present with both the superficial, bright red component and a deeper, blue nodularn component
Infantile hemangioma • The natural history of infantile hemangiomas is characteristic. Itis notable for a period of growth (the proliferative phase), a periodof stability (the plateau phase), and a period of spontaneous regression (the involutional phase). • The majority of infantile hemangiomas first become evident at 2–3 weeks of life, with potential continued growth until around 9–12 months of age. • The majorty of growth, however, occurs during the first 5 months of age, and in those that continue to grow beyond this age, the growth rate is markedly slower.
Infantile hemangioma • Occasional lesions have a proliferative phase that lasts for >1 year, sometimes as long as 18–24 months. • Deep hemangiomas tend to exhibit both a delayed onset of growth, as well as a sustained, longer growth phase. • The onset of the involutional phase, which is difficult to predict in any given patient, is marked by a color change from bright red to dull red, purple, or marked by a color change from bright red to dull red, purple, or gray (for superficial lesions)
Infantile hemangioma • It is estimated that completed involution of infantilehemangiomasoccurs at a rate of 10% per year, such that 30% haveinvolutedby 3 years of age; 50% by 5 years of age; 70% by 7 yearsof age, and >90% by 9–10 years of age. • However, it shouldbe remembered that involution does not necessarily imply totallynormal skin. • Thesepossibilities must be explained thoroughly to the parents of patientswith infantile hemangioma.
Infantile hemangioma • Treatment decisions regarding an infantile hemangioma must incorporate many factors. • These include the size and location of the lesion or lesions , the age of the patient and growth phase of the hemangioma, associated findings, and the perceived potential for psychosocial distress both for parents and for the patient later in life. • The major goals of management should be to prevent or reverse life-or function-threatening complications; prevent disfigurement; minimize psychosocial stress; avoid overly aggressive procedures; and adequately prevent or treat ulceration in order to minimize infection, pain, and scarring.
Infantile hemangioma • Corticosteroids are the traditional mainstay of therapy for hemangiomasrequiring treatment. • They are most often used in the oral form, although both intralesional and topical preparations may be useful. • Intralesional corticosteroids are useful for localized lesions. • Several injections may be necessary, and periocular lesions shouldbe treated only by a physician experienced in their administration,
Infantile hemangioma • Topical corticosteroid therapy with clobetasol propionate (a potent, class 1 topical steroid) may be useful for localized hemangiomas. • In the authors’ experience,this therapy is most useful for macular or very thin plaque heman-giomas in the early proliferative stage • This medication should beused cautiously with attention to the risks of atrophy, ocular toxic-ity, and adrenal suppression.
Infantile hemangioma • Oral corticosteroids are the traditional ‘gold standard’ for com-plicated infantile hemangioma treatment, although their mecha-nism of action is poorly understood. • They are most useful duringt he proliferative phase, and are generally administered in dosages ranging from 2 to 4 mg/kg per day of prednisolone or prednisone. • Thistherapy is usually continued for several months, with gradual tapering as tolerated. • If corticosteroids are tapered too quickly, rebound growth and adrenal suppression may occur. • The goals of decreased hemangioma growth or partial shrinkage must be balanced by the risks of long-term therapy. • Common side-effects include irritability,weight gain, hypertension, and gastrointestinal upset.
Infantile hemangioma • An evolving therapy for infantile hemangioma is propranolol. • The mechanism of action of propranolol in this setting isunclear. • It is most often started at around 0.5 mg/kg per day, with the dose gradually titrated up to 2 mg/kg per day, divided into two to three doses daily. • Potential side-effects include hypotension,bradycardia, bronchospasm, hypoglycemia and hypothermia, and this agent should be administered under close supervision with attention to these possible toxicities.
Infantile hemangioma • Pulsed-dye laser (PDL) therapy may be useful in the treatment of ulcerated hemangiomas. • This laser emits a wavelength of light specific for oxyhemoglobin, thus imparting specificity for vascular structures (’selective photothermolysis’). Since the light penetrates only 1 mm of depth in the skin, this modality is generally not helpful for non-ulcerated, elevated, or nodular lesions. • With ulcerated lesions, though, it is useful in accentuating reepithelializationand decreasing pain. • The choice of PDL therapy must be individualized to the patient, and occasional patients may show noresponse or even worsening with this modality. • PDL therapy mayalso be useful for residual surface vascularity following hemangiomainvolution.
Vascular malformations • The salmon patch (nevus simplex) is the most common vascular esion of infancy. • It occurs in 30–40% of all newborns and appearsas a flat, dull pink, macular lesion on the posterior neck and scalp, glabella , forehead, upper eyelids, and occasionally the nose or nasolabial regions • No treatment is necessary, since 95% of facial salmon patches fade within the first 1–2 years of life.
Nevus flammeus, or port-wine stain (PWS), • Nevus flammeus, or port-wine stain (PWS), is a congenital capillary malformation that may occur as an isolated lesion or in association with a variety of syndromes. • These lesions present as macular (non-palpable) stains with a pink to dark red color. • Although an early PWS may be indistinguishable from an infantile hemangioma, these lesions are usually distinguished by their congenital presence and their static nature, without the rapid proliferation and thickening that characterizes hemangiomas during the first months of life. • PWS may darken progressively over many years, and occasional lesions develop secondary proliferative(pyogenic granuloma-like) vascular blebs on their surface . • They may also become somewhat thickened and raised later in life. • Port-wine stains are often, but not always, unilateral and the most common site of involvement is the face, although they may occur on any cutaneous surface.
Nevus flammeus, or port-wine stain • PWS lesions show little tendency toward spontaneous improvement or involution, • Laser therapy has revolutionized the treatment of these lesions, and the flashlamp-pumped tunable pulsed-dye laser (PDL) is the most accepted laser for PWS treatment. • PDL allows the targeting of short bursts of energy at intravascular hemoglobin (because of the specific wavelength of the emitted light)within the lesional vessels, while sparing other tissue components and thus allowing for precise therapy. • Treatment of PWS with PDL is usually performed in conjunction with local or general anestheia, depending on the size and location of the lesion and the age of the patient. • Some smaller lesions can be treated without the need for anesthesia. • PDL therapy is usually performed over several sessions, separated in time by 6–8 weeks, and can be quite effective in lightening these lesions, thereby minimizing their cosmetic and psychosocial significance109
Nevus flammeus, or port-wine stain • Some authors have reported optimal treatment response in patients<1 year of age, whereas others have found no evidence that treat-ment during early childhood is more effective than treatment at alater age. • In general, lesions over bony areas of the face (i.e.,the forehead), lateral cheeks, chest and proximal arms seem to respond best to PDL therapy, while those over the mid-face and distal extremities respond less. • PWS of the central face may not respond as well, given the deeper vessels which may escape the effect of the PDL.
Sturge–Weber syndrome • Sturge–Weber syndrome (SWS, encephalofacial or encephalotrigeminalangiomatosis) is a neuroectodermal syndrome characterzedby a PWS in the distribution of the first (ophthalmic) branch of the trigeminal nerve (V1) in association with leptomeningealangiomatosis (presenting usually with seizures) and glaucoma. • There are rare reports of patients with classic brain and ophthalmic findings of SWS in the absence of facial PWS.
Port wine stain on face beforetreatment. (b) Portwine stain on face after pulsed dye laser treatment
Nevus flammeus, or port-wine stain • The potassium titanyl phosphate (KTP) laser emits greenlight at 532 nm. • High fluences are available with this laser and the pulse durations may be more appropriatefor some PWSs. • The KTP laser has been shown to produce further lightening in PDL-resistant lesions . • In this study, 30 patients with PWS that had failed to lighten after at least five treatments with the PDL at 0.5-ms pulse widths were treated with the KTP laser. Fluencesrangedfrom 18 to 24 J cm−2 with pulse widths of 9–14 ms. • Five patients (17%) showed more than 50% response. • In general, patients preferred the KTP laser because there was less discomfort and purpura. • However, two patients (7%)developed scarring.
Nevus flammeus, or port-wine stain • A study comparing the PDL with a frequency-dou-bled Nd:YAG laser showed similar response rates among43 patients; however, a substantially higher scarring ratewith the 532-nm Nd:YAG laser was noted [13]. • Longer-wavelength lasers such as the alexandrite(755 nm) and Nd:YAG (1,064 nm) may have a role in PWS treatment. In the milli second modes these lasers have been widely used for hair removal and leg vein telangiectasia. • These lasers may be particularly useful in the treatment of bulky malformations and mature PWSs, lesions that are typically more resistant to PDL because of the predominance of larger and deeper vessels and higher content of deoxygenated hemoglobin.
Nevus flammeus, or port-wine stain • Yang et al. [22] treated 18 patients with PWSs,comparing a 595-nm PDL to a long-pulsed Nd:YAGlaser with contact cooling. • Similar clearance rates were achieved. • Patients preferred the Nd:YAG laser because of the shorter recovery period between treatments.
Nevus flammeus, or port-wine stain • Intense pulsed light (IPL) has also been used to treatPWSs. Unlike laser systems, these flash lamps producenoncoherent broadband light with wavelengths in therange of 515–1,200 nm and permit various pulsewidths. • Filters are used to remove unwanted wave-lengths.