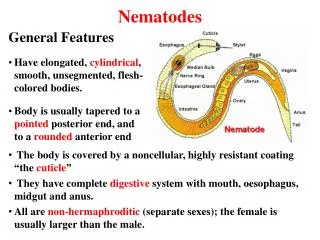
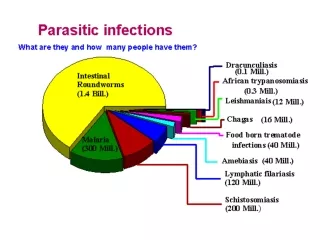
Tissue Nematodes
Tissue Nematodes. II MBBS Dr Ekta Chourasia Microbiology. Classification – Tissue Nematodes. Lymphatic. Wuchereria bancrofti. Brugia malayi. Brugia timori. Subcutaneous. Loa loa (african eye worm). Onchocerca volvulus (blinding filaria). Dracunculus medinensis (thread worm).

Tissue Nematodes
E N D
Presentation Transcript
Tissue Nematodes II MBBS Dr Ekta Chourasia Microbiology
Classification – Tissue Nematodes Lymphatic Wuchereria bancrofti Brugia malayi Brugia timori Subcutaneous Loa loa (african eye worm) Onchocerca volvulus (blinding filaria) Dracunculus medinensis (thread worm) Conjunctiva Loa loa Dr Ekta, Microbiology
Wuchereria bancrofti (Filarial worm) Definitive host Man Intermediate host Female Culex, Aedes or Anopheles mosquito Infective form Third stage larva Mode of transmission Inoculation – bite of mosquito Site of localization Lymphatics / lymph nodes of man Geographical distribution India, China, Far East, Africa, South & Central America Dr Ekta, Microbiology
Life cycle Dr Ekta, Microbiology
Clinical features • Infection - Wuchereriasis/ Lymphatic filarisis/ Bancroftian filariasis • Pathogenic states are produced only by adult worm (living/ dead) – classical filariasis Occult filariasis – lesions produced by microfilaria • Clinical states in classical filariasis can be classified as: • Asymptomatic ( in endemic areas) • Inflammatory • Obstructive • Tropical pulmonary eosinophilia (occult filariasis) Dr Ekta, Microbiology
1. Inflammatory stage • Lymphadenitis – LNs of groin & axilla • Lymphangitis – lymphatics of extremities, testicles & epididymis • Filarial fever – high grade fever with chills Fever subsides in 7-10 days but such inflammatory attack recurs every month • Repeated attacks – damage lymphatics – chronic lymphoedema Dr Ekta, Microbiology
Causes of lymphangitis • Mechanical irritation – movement of adult parasite inside lymphatics • Liberation of metabolites of growing larvae • Secretion of toxic fluid by fertilized female worms • Absorption of toxic products liberated from dead worms Dr Ekta, Microbiology
2. Obstructive stage • Lymphatic obstruction – occurs with the death of worms • Causes of obstruction – • Blocking of lumen by dead worms • Excessive proliferation & thickening of walls of lymphatic vessels • Fibrosis of lymphatic vessels Dr Ekta, Microbiology
3. Complications of Lymphatic Obstruction • Elephantiasis of organs like leg, scrotum, penis, vagina, breast, arm etc – fibrotic thickening of skin & subcutaneous tissue • Lymphangiovarix – dilatation of afferent lymphatics. • Rupture of Lymphangiovarix into urinary tract – chyluria • Hydrocele Dr Ekta, Microbiology
Lymphatic filariasis Dr Ekta, Microbiology
4. Tropical Pulmonary Eosinophilia • Hypersensitive reaction to microfilarial Ags. • Microfilariae trapped in alveoli – eosinophil rich intra alveolar infiltration • C/F – paroxysmal cough, wheezing, wt loss, low grade fever, LNpathy, eosinophilia. • Excessive rise in antifilarial Ab titres & serum IgE levels. • Drug of choice – DEC • Symptoms resolve in 3 to 7 days of therapy. Dr Ekta, Microbiology
Classical v/s Occult filariasis Dr Ekta, Microbiology
Laboratory diagnosis • Specimen- blood collected at night, preferably capillary blood from ear lobes, chylous urine, hydrocele fluid, exudate from lymphangiovarix • Microscopic examination – wet mount or stained with giemsa: sheathed microfilaria with no nuclei at tail tip Dr Ekta, Microbiology
Laboratory diagnosis • Concentration techniques – for capillary blood, venous blood (Knott’s technique) • DEC provocation test – 100 mg of DEC orally, examine peripheral blood smear after 30 to 45 minutes • Serology – using non specific Ags • Passive hemagglutination test • Fluoresecent ab test • ELISA Dr Ekta, Microbiology
Treatment DEC (Diethylcarbamazine) – microfilaricidal: 6mg/ kg/day for 2-3 weeks Elevation of the affected limbs, use of elastic bandages & local foot care – reduces symptoms of lymphatic obstruction Surgical treatment of hydrocele Prevention Destruction of mosquitoes Protection against mosquito bites Treatment of carriers Dr Ekta, Microbiology
Brugia sps • Two species infect humans : B.malayi & B.timori • Causes lymphatic filariasis • Transmitted by Mansonia & Anopheles species of mosquitoes • Life cycle, pathogenesis, clinical features, diagnosis & treatment – similar to W. bancrofti, with a following differences • Children commonly affected • Rapid development of signs & symptoms • Elephantiasis affect lower extremities • Chyluria & hydrocele rare • Microfilaria : sheathed with 2 widely spaced nuclei & blunt tip at tail end. Dr Ekta, Microbiology
Onchocerca volvulus (Blinding filaria – 2nd most common cause of infectious blindness) Definitive host Man Intermediate host Black flies (simulium) Infective form Larva Mode of transmission Inoculation Site of localization Subcutaneous tissue, dermis & eye Dr Ekta, Microbiology
Clinical features • Incubation period - 10 to 12 months • Eosinophilia and urticaria. • Nodular and erythematous lesions (Onchocercomata) in the skin and subcutaneous tissue • Photophobia, lacrimation, keratitis and blindness – due to trapping of microfilaria in the cornea, choroid, iris and anterior chambers. Dr Ekta, Microbiology
Diagnosis & Treatment • Nodular biopsy – adult worm • Skin snip – unsheathed microfilaria with no nuclei • Treatment – Ivermectin, surgical removal, DEC in non ocular onchocercosis Dr Ekta, Microbiology
Loa loa (African eye worm) Definitive host Man Intermediate host Chrysops (deer fly) Infective form Larva Mode of transmission Inoculation Site of localization Subcutaneous & deep connective tissue Dr Ekta, Microbiology
Clinical features • Subcutaneous swelling – Calabar or fugitiveswelling, measuring 5 to 10 cm, marked by erythema and angioedema, usually in the extremities • Migrating worm in subconjunctival tissue Dr Ekta, Microbiology
Diagnosis & Treatment • Peripheral blood smear - Sheathed microfilaria with nuclei upto rounded tail tip • Isolation of worms from the conjunctiva or subcutaneous biopsy • Treatment - Ivermectin, surgical removal, DEC (effective against adult & microfilaria) Dr Ekta, Microbiology
Dracunculus medinensis (Guinea Worm) Adult worms Male 2 to 4 cm Female 70 –120 cms, viviparous Definitive host Human Intermediate host Cyclops Infective form Larva inside Cyclops Mode of transmission Ingestion of water contaminated with cyclops Site of localization Subcutaneous tissue Dr Ekta, Microbiology
Clinical Features • Disease – Dracunculosis • Clinical features develop an year after infection following the migration of worm to the subcutaneous tissue of the leg • Blister formation – rupture of blister when in contact with water - ulceration – release of larvae by adult female worm • Secondary bacterial infection of ulcer Dr Ekta, Microbiology
Diagnosis & Treatment • Detection of adult worm – when it appears at the surface of skin • Detection of larva – in milky fluid released by worm on exposure to water • Radiology – calcified worm in deeper tissues • Treatment – • Thiabendazole/ Metronodazole – symptomatic relief, easy removal of worm • Gradual extraction of worm by winding of a few cms on a matchstick per day, over 3 to 4 weeks • Surgical excision Dr Ekta, Microbiology
Prevention • Provision of safe water supply • Education to discourage people from entering water source • Filtering water through a double folded cloth • Boiling water before drinking • Discouraging the use of step wells Dr Ekta, Microbiology