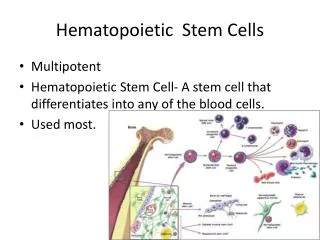
Hematopoietic Malignacies
Hematopoietic Malignacies. Plasma Cell dyscrasias (Lymphomas). Common Issues in HCs. HC: ~ 10% of all malignacies (incidence/death) Lymphomas: 4% of all cancers mobility of cells genetic instability clonal expansion potential. HC: 45% NHL HC: 12% HL HC: 14% Myelomas HC: 29% Leukemias.

Hematopoietic Malignacies
E N D
Presentation Transcript
Hematopoietic Malignacies Plasma Cell dyscrasias (Lymphomas)
Common Issues in HCs • HC: ~ 10% of all malignacies (incidence/death) • Lymphomas: 4% of all cancers • mobility of cells • genetic instability • clonal expansion potential
HC: 45% NHL • HC: 12% HL • HC: 14% Myelomas • HC: 29% Leukemias
Historical notes 1750s: Robert Virchow: “leukemia” 1850s: Thomas Hodgkin: H.Disease 1950s: HD as Hlymphoma 1950s: Peter Nowell+David Hungerford: abnormal short chromosome 22 in CML 1970s: Jenat Rowley, Chicago, increased chromosome 9 (22-> 9 translocation) + multiple other defects lymphoblastic lymphomas / lymphocytic lymphomas cancer stem cells (AML, tumor transfer studies)
oncogenesis • Genetic (translocations / recurring translocations, mutations • environmental carcinogens (benzene, radiation) • secondary to intensive RxT, ChemoTher (for a primary cancer / in preparation for BMT or HCT)
Clinical terms • Acute / chronic • high grade (transformed precursor cells); T1/2 ~ 24 months • medium / low grade (more mature phenotypes, 2 - 5 years) • clinical responses: complete remission (>4 weeks) / relapse; refractory to treatment / salvage therapy; LTS/residual disease in > 5 years
therapeutics • Autologous HCT (G-CSF, leukaferesis, CD34+) • allogeneic BM, HLA-matched • biologicals: IFNalpha, mAbs anti CD19, CD20, CD22 (ADCC, complement CML), immunotoxins (diphteria toxin - IL2 for IL-2R+ T lymphomas; radiolabelling Yttrium 90, Iodine 131
Plasma cell dyscrasias • M protein (paraprotein) • Monoclonal Gammapathy of Undetermined Significance (MGUS) • 1% of age > 40y • 70% asymptomatic; transitory • 25%: mild anemia => myelomas or B cell lymphomas
Waldenstrom Macroglobulinemia large quantities of IgM paraproteins viscous blood => vision / neurologic signs accumulation of tumors BM, spleen, lymph nodes (>40%) anemia hemorrhaging cutaneous lesions (cells / deposits) unlike lymphomas: not producing osteoclast activating factors; BM lesions less than 10% good response to purine analogues (cladribine)
Myeloma • Often arise from preexisting MGUS by additional mutations • anemia • state of immunosuppression, infections • hypercoagulability • circulatory difficulties, pulmonary function reduced • neurological signs • many cases: excess of Bence Jones proteins
Tam-Horshfall protein binding - aggregates promoting hypercalciuria and hypercalcemia; interstitial nephritis (kidney failure) • 4/100 000 (age, sex, race); HLA-Cw2 • ionizing radiation • classification: multiple criteria • DEREGULATION in CYTOKINES
IL-6 appear to autodrive the cancer STAT-3: upregulation of Bcl-xL; upregulation Myeloid Cell Factor 1 (MCL-1, essential for tumor cell survival) induces VEGF in myeloma cells: promotes angiogenesis, migration of tumor cells, IHIBITS Ag presentation by DCs IL-6+MIP-1a+IL-1b+TNF => BM stromal cells produces OPGL, master regulator of osteoclastogenesis IL-2+IL-7+IL-11+Lta+GM-CSF => suppresses IgG, Th, NK TGFb: autocrine loop for IL-6 secretion IGF-1 of BM stromal cells=> PI3K / PKB(AKT) = > survival
Genetics: many abnormalities Trisomy 6, 9(with more favourable prognosis) and 3, 5, 7, 11, 15, 19 13q deletions very poor prognosis 70%: Cdk mutations p15, p16 Cdk inhibitor / hypermethylation Ras oncogene activation (late stages); p53 (late stages)
Early: translocation Ig H locus FGFR3 gene, 4p16 => fusion product blocks caspase-3 apoptosis IRF4 gene 67p21 cyclin D3 gene 6p21 Bcl-1 gene at 11q13 common upregulation of Bcl-2, Bcl-xL deletions of 13q14 (Rb tumor suppressor gene)
Treatment: difficult 5 years survival < 30% early stages : INDOLENT alkylating agents (melphalan) + prednison alternative: dexamethasone, vincristine, thalidomide, adriamycin Thalidomide: activates caspase 8; blocks IL6, angiogenetic activity BORTEZOMIB (Velcade) proteosomal inhibitor, limits the catabolism of ubiquitinated proteins, including I-kB=> block IL6, induces apoptosis, decreases VEGF IGNa: remission, but not longer survival biphosphonates (osteoclast inhibitors: zolendronate, pamidronate)