Download
1 / 9
90 likes | 99 Vues
Cerebellar Direct Current Stimulation (ctDCS) for the treatment of phantom limb pain Bocci Tommaso 1,2 , De Carolis G. 3 , Mansani F. 1 , De Rosa A. 1 , Ferrucci R. 2 , Priori A. 2 , Valeriani M. 4 , Sartucci F. 1,5

E N D
Cerebellar Direct Current Stimulation (ctDCS) for the treatment of phantom limb pain Bocci Tommaso 1,2, De Carolis G.3, Mansani F.1, De Rosa A.1, Ferrucci R. 2, Priori A. 2, Valeriani M. 4, Sartucci F.1,5 1 Department of Health Sciences, University of Milan, Milan, Italy; 2 Department of Clinical and Experimental Medicine, University of Pisa; 3Pain Therapy Unit, University of Pisa, Pisa, Italy; 4 Division of Neurology, Ospedale Bambino Gesù, Rome, Italy; 5Neuroscience Institute, National Research Council, Pisa, Italy
From bench to bedside: putative pathways What did we learn from MRI studies? Moulton et al., Brain Res Rev 2010 Borsook et al., Cerebellum 2008; Dimitrova et al., J Neurophysiol 2003; Plogahus, Science 1999
A new target for pain treatment in humans: the cerebellum Bocci et al., Restor Neurol Neurosci 2015 Bocci et al., Cerebellum 2016 Parazzini et al., Clin Neurophysiol 2013
Central sensitization and chronic pain syndromes: the “red flags” for putative therapies Spinalmechanisms: Phenotipicswitch in the expressionofneuropeptides • Supra-spinalmechanisms: • Reorganizationofsensorimotormaps • ThalamocorticalDysrhythmia Hsieh et al., Pain 2015 Suzuki&Dickenson, Neurosignals 2006
tDCS and phantom limb pain (PLP) Is it really effective? tDCS over the primary motor cortex (Bolognini et al., J Pain 2015)
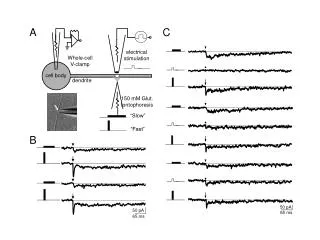
Experimental Protocol 1. ClinicalScales 2. LEPs (nociceptive threshold, N1 and N2/P2 amplitude/latency) 3. fMRI 1. ClinicalScales 2. LEPs (nociceptive threshold, N1 and N2/P2 amplitude/latency) 3. fMRI 1. ClinicalScales 2. LEPs (nociceptive threshold, N1 and N2/P2 amplitude/latency) 3. fMRI T0 T1 (immediately after ctDCS) T2 and T3 (after two and three weeks ctDCS completion) Cerebellar tDCS (sham or anodal), five days a week (2.0 mA, 20’ per day).
Clinical scores Bocci et al., Cerebellum 2019
Neurophysiological outcome Bocci et al., Cerebellum 2019
Conclusions • Anodal stimulation significantly improves both painful and non painful phantom limb sensations, dampening LEP amplitudes over time; • Cerebellar polarization may be useful for the treatment of pain syndromes; it may act not only on spinal nociceptive neurons, but also on wide-range cortical networks of the pain matrix, thus influencing pain experience through top-down and bottom-up mechanisms.