Download
1 / 39
390 likes | 466 Vues
Explore the absorption of drugs through the cell membrane, mechanisms, and factors affecting absorption. Learn about transcellular and paracellular transport, and the role of lipid bilayers and proteins in drug absorption.

E N D
CONTENTS • Introduction of absorption • Structure of the Cell Membrane • Gastro intestinal absorption of drugs • Mechanism of Drug absorption • Factors affecting drug absorption • Absorption of drugs from non-per oral routes.
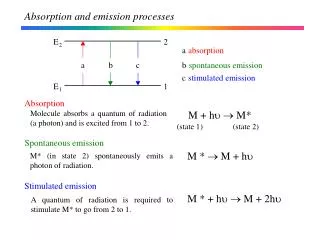
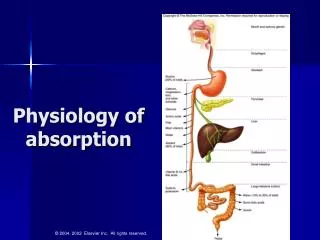
INTRODUCTION OF ABSORPTION • Defined as the process of movement of unchanged drug from the site of administration to the site of measurement i.e., plasma • Effectiveness can be assessed by measuring concentration at the site of action, which is difficult • There always exist a correlation between the plasma concentration of a drug & the therapeutic response
Not only the magnitude of drug that comes into the systemic circulation but also the rate at which it is absorbed is important Therapeutic success of a rapidly & completely absorbed drug. Minimum effective conc. Plasma Drug Conc. Therapeutic failure of a slowly absorbed drug. Sub therapeutic level Time
CELL MEMBRANE • The plasma membrane is a flexible yet sturdy barrier that surrounds & contains the cytoplasm of a cell. • Cell membrane mainly consists of: 1. Lipid bilayer • phospholipid • Cholesterol • Glycolipids. 2. Proteins • Integral membrane proteins • Lipid anchored proteins • Peripheral Proteins
It consists of two back to back layers of Lipids: Phospholipid, Cholesterol, Glycolipids. PHOSPHOLIPIDS : Principal type of lipid in membrane about 75 %. Polar region is hydrophilic and non polar region is hydrophobic. Non polar region contain two fatty acid chain. One chain is straight fatty acid chain. (Saturated) &Another chain has cis double bond which are Unsaturated .
CHOLESTEROL • Amount in membrane is 20 %. • Inserted in membrane with same orientation as phospholipids molecules. • Polar head of cholesterol is aligned with polar head of phospholipids. Function: • Immobilize first few hydrocarbons groups of phospholipids molecules. • Prevents crystallization of hydrocarbons & phase shift in membrane
GLYCOLIPIDS • Presents about 5% of total lipids. • Carbohydrate groups form polar “head”. • Fatty acids “tails” are non polar. • Present in membrane layer that faces the extracellular fluid. • This is one reason due to which bilayer is asymmetric. Functions: Protective Insulator Site of receptor binding
INTEGRAL PROTEINS • Also known as “Transmembrane protein”. • Have hydrophilic and hydrophobic domain. • Hydrophobic domain anchore within the cell membrane and hydrophilic domain interacts with external molecules. • Hydrophobic domain consists of one, multiple or combination of α – helices and ß – sheets of protein . • Ex: – Ion Channels, Proton pump.
LIPID ANCHORED PROTEIN • Covalently bound to single or multiple lipid molecules. • Hydrophobically inert into cell membrane & anchor the protein. • The protein itself is not in contact with membrane. • Ex.: G Proteins (guanine nucleotide-binding proteins).
PERIPHERAL PROTEINS • Attached to integral membrane proteins OR associated with peripheral regions of lipid bilayer. • Have only temporary interaction with biological membrane. • Once reacted with molecule, dissociates to carry on its work in cytoplasm. • Ex.: Some Enzyme, Some Hormone
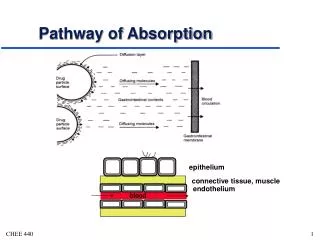
MECHANISMS OF DRUG ABSORPTION • 1.Transcellular/Intracellular Transport • Defined as the passage of drugs across the GI epithelium(lipoidal barrier) this is the major obstacle to drug absorption • It is the most common pathway for drug transport • Movement across the intracellular space (cytosol)
I . Passive Transport Processes : This transport processes does not require energy other than that of molecular motion (Brownian motion) they pass through the lipid bilayer • Passive diffusion. • Pore transport. • (c) Ion-pair transport. • (d) Facilitated or mediated diffusion • II .Active Transport Processes: These transport processes requires energy from ATP to move drug molecules from extracellular to intracellular site • Primary active transport. • (b) Secondary active transport • (i) Symport (co-transport) • (ii) Antiport (counter-transport)
2. Paracellular /Intercellular Transport • The transport of drugs through the junctions between the GI epithelial cells. This pathway is of minor importance in drug absorption. • I. Permeation through tight junctions of epithelial cells :Basically occurs through openings which are little bigger than the aqueous pores. Ex. Insulin and Cardiac glycosides. • II. Persorption: Permeation of drug through temporary openings formed by shedding of two neighbouring epithelial cells into the lumen.
3. Vesicular or Corpuscular Transport (Endocytosis) These are energy dependent processes that involve transport of substances within vesicles into a cell. This process is classified as transcellular 1. Pinocytosis 2. Phagocytosis
Types • Passive diffusion • Pore transport • Carrier- mediated transport a) Facilitated diffusion b) Active transport • Ionic or Electrochemical diffusion • Ion-pair transport • Endocytosis
PASSIVE DIFFUSION Also known as non-ionic diffusion. Absorption of 90% of drugs. The driving force for this process is the concentration or electrochemical gradient. It is defined as the difference in the drug concentration on either side of the membrane.
characteristic of passive diffusion: Down hill transport Greater the surface area & lesser the thickness of the membrane, faster the diffusion. Equilibrium is attained when the concentration on either side of the membrane become equal. Greater the membrane/ water partition coefficient of drug, faster the absorption. Follows first order Kinetics
Passive diffusion process is energy independent but depends more or less on the square root of the molecular size of the drugs. • The mol. Wt. of the most drugs lie between 100 to 400 Daltons which can be effectively absorbed passively.
Pore Transport • Also known as convective transport, bulk flow or filtration. • Important in the absorption of low mol. Wt. (less than 100) Low molecular size (smaller than the diameter of the pore) & generally water-soluble drugs e.g. urea, water & sugars • Occurs through narrow, aqueous filled channels or pores in the membrane structure. • Driving force for is the hydrostatic or the osmotic pressure difference across the membrane.
Carrier Mediated Transport Mechanism • Involves a carrier (a component of the membrane) which binds reversibly with the solute molecules to be transported to yield the carrier solute complex • Complex transverses across the membrane to the other side where it dissociates to yield the solute molecule • The carrier then returns to its original site to accept a fresh molecule of solute.
There are two types of carrier mediated transport system a) Facilitated diffusion b) Active transport Characteristics: • Carrier protein always has an uncharged outer surface. • Carriers are bidirectional. • Transport process is structure specific – lock and key mechanism.
Substance having similar structure as structure specific nutrients gets transported, false nutrient. • Specialized area within GIT where there are abundant numbers of carriers. Such an area rich in carriers is called Absorption Window. • Carriers are limited & gets saturated • Initially the process is fast and follows first order kinetics. • Carrier gets saturated with time & the process becomes concentration independent i.e., follows zero order kinetics.
Facilitated Diffusion This mechanism involves the driving force i.e concentration gradient. Down-hill transport, therefore the process is not inhibited by metabolic poisons that interfere with energy production. Limited importance in the absorption of drugs. Eg. entry of glucose into RBCs & intestinal absorption of vitamins B1 & B2. Gastro-intestinal absorption of vitamin B12 with an intrinsic factor (IF), a glycoprotein produced by the gastric parietal cells.
Active Transport The driving force is against the concentration gradient or uphill transport. Hence energy is required it can be inhibited by metabolic poisons that interfere with energy production. If drugs (especially used in cancer) have structural similarities to such agents, they are absorbed actively. Faster than passive diffusion
Primary active transport • Requires direct ATP. • Transfers only one ion/molecule in one direction- Uniport. • Ex: absorption of glucose • Ion transporters • Types organic anion and cations transporters. • Ex: ATP- driven ion pump or H+ pump. • ABC(ATP- binding cassette ) transporter: • transporting small foreign molecules • Ex: ABC transporter is P- glycoproteins which transports hydrophobic drugs.
Secondary active transport • The energy required in transporting an ion aids transport of another ion/ molecule (co-transporter/coupled transport) • Symport (co-transport) : • Movements is in the same direction. • Ex: Na+- glucose symporter uses potential energy of the Na+ concentration gradient to more glucose against concentration gradient. • Antiport (counter transport): • Movement in opposite direction. • Ex: expulsion of H+ ions using Na+ ion gradient in kidneys.
Ion Pair Transport This mechanism explains the absorption of drugs which ionize at all pH condition. Quaternary ammonium compounds and sulfonic acids
Transport of charged molecules due to the formation of a neutral complex with another charged molecule carrying an opposite charge. • Drugs form reversible neutral complexes with endogenous ions. e.g. mucin of GIT • Such neutral complexes have both the required lipophilicity as well as aqueous solubility for passive diffusion.
Endocytosis • Involves engulfing extracellular materials within a segment of the cell membrane to form a saccule or a vesicle • Hence also called as corpuscular or vesicular transport. • which is then pinched off intracellularly. • Types • Phagocytosis • Pinocytosis • Transcytosis
PINOCYTOSIS • Uptake of fluid solute. • A form of endocytosis in which liquid are brought into the cell in the form of small vesicles which subsequently fuse with lysosomes to hydrolyze & break down. • This process requires energy in the form of (ATP). • Cell drinking • Absorption of oil soluble vitamins & in the uptake of nutrients Polio vaccine and large protein molecules are absorbed by pinocytosis
Exocytosis • Reverse of endocytosis • Used for expelling wastes, secreting substances • Vesicle moves to plasma membrane, breaks open, releasing substance. Transcytosis It is a phenomenon in which endocytic vesicle is transferred from one extracellular compartment to another.
Combined absorption mechanisms Absorption mechanism Drugs Absorbed Passive Most drugs having high Diffusion lipophilicity & Mw in the range 100-400 Pore Water-soluble drugs of Transport MW less than 100 Ion-Pair Drugs that ionise at all Transport pH conditions absorbed after complexing with oppositely charged ions Carrie-Mediated Structure-specific drugs Transport with affinity for carriers transported from specific sites Endocytosis Macromolecular nutrients & drugs as solid particles or oily droplets