LIPIDS 101
LIPIDS 101. Ulrich K. Schubart JMC AECOM. Physiology of Lipids and Lipoproteins Lipoprotein Disorders. COMPOSITION OF PLASMA LIPOPROTEINS. 2. 7. 5. 6. 19. 22. 18. 22. 50. 40. 5. 22. 33. 6. 55. 86. Chylomicrons VLDL LDL HDL.

LIPIDS 101
E N D
Presentation Transcript
LIPIDS 101 Ulrich K. Schubart JMC AECOM
Physiology of Lipids and Lipoproteins • Lipoprotein Disorders
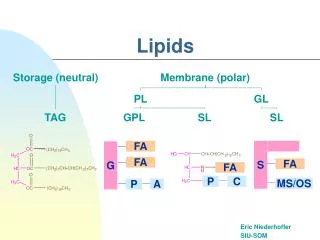
COMPOSITION OF PLASMA LIPOPROTEINS 2 7 5 6 19 22 18 22 50 40 5 22 33 6 55 86 ChylomicronsVLDLLDL HDL Chylomicrons VLDL LDL HDL Density g/ml 0.93 0.93-1.006 1.019-1.063 1.063-1.25 Size (nM) 75-1200 30-60 18-25 9-12 Cholesterol/cholesteryl esters Phospholipid Protein Triglyceride Bilheimer. Textbook of Internal Medicine. 1989:2139-44
Exogenous Pathway (Chylomicron metabolism) Apo E Apo E Chylomicron Remnant Liver B48 CE B48 LPL CE CE TG TG C-II Intestines Remnant Receptor Fatty acids
Apo E Apo E Endogenous Pathway (VLDL metabolism) Liver VLDLRemnant LDL (VLDL/IDL) B100 B100 B100 CE Remnant Receptor LPL CE CE CE TG TG C-II Fatty acids
Basic Pathways in LDL Regulation apo B-100 apo E VLDL VLDL PRODUCTION LIPOLYSIS apo C SHUNT PATHWAY Liver VLDL Remnant LDL CLEARANCE CONVERSION Other sites LDL
Familial Hypercholesterolemia • Autosomal Dominant Inheritance • LDL Receptor Deficiency: • - Heterozygous (1/500) • - Homozygous (1/1,000,000) • LDL Cholesterol Increased • - Heterozygous 2 times (>250 mg/dl) • - Homozygous 4-6 times elevated • Familial Defective apoB is an exact phenocopy (note this is NOT Familial Combined HLD)
Liver ChyloVLDLRemnants LDL apoB CE apoB LPL CE CE TG TG LDL-R C-II Apo E Apo E Fatty acids B100 Familial Hypercholesterolemia
Familial Hypercholesterolemia: Clinical Manifestations • Severe Hypercholesterolemia (LDL>250 mg/dl) • - Atherosclerotic vascular disease • Premature CHD • Xanthelasma/ Corneal Arcus as young adults • Tendon Xanthomas • Arthritic type pains in joints • Family History of premature CHD
Liver ChyloVLDLRemnants LDL apoB CE apoB LPL CE CE TG TG LDL-R C-II Apo E Apo E Fatty acids B100 Familial Hypercholesterolemia: Ligand Defective ApoB
Familial Combined Hyperlipidemia Common (1/100) Autosomal dominant pattern of inheritance Variable lipoprotein pattern in individual and family Multiple Phenotypes (IIa, IIb, IV, V) Pathophysiology: overproduction of apoB-100 particles CHD risk is increased
VLDL Remnant LDL (VLDL/IDL) B100 CE B100 CE LDL-R TG TG Apo E Apo E Familial Combined Hyperlipidemia (HyperapoB) Liver LPL B100 CE CE C-II Fatty acids
Familial (Type I) Hyperlipoproteinemia/Chylomicronemia • Rare (1/1,000,000) • Recessive inheritance • Triglycerides > 1000 mg/dl with usual diet • Presents in childhood, especially puberty in girls • Pathophysiology: absence of lipoprotein lipase or apo C-II • Complications: pancreatitis, xanthomatosis, hepatosplenomegaly
CE TG LDL-R Apo E Apo E Familial (Type I) Hyperlipoproteinemia/Chylomicronemia Chylo/VLDLRemnants LDL (VLDL/IDL) Liver apoB apoB B100 LPL CE CE CE TG C-II Fatty acids
Remnant Removal Disease • Synonyms: Familial Dysbetalipoproteinemia, Type III hyperlipoproteinemia, Broad beta disease • Uncommon: 1/1000 – 1/5000 • Requires apo E2/E2 (1/100) + second defect for clinical expression • Pathophysiology: impaired clearance of apoB/E remnant particles by the remnant receptor • Chylomicron and VLDL (-VLDL) remnants accumulate • Diagnosis: VLDL-C/TG >0.3; broad -band on EP • CHD and peripheral vascular disease • Palmar and tuberoeruptive xanthomata _
Liver ChyloVLDLRemnants LDL apoB CE apoB B100 LPL CE CE LDL-R TG TG C-II Apo E2/E2 Apo E Fatty acids Remnant Removal Disease (Type III Hyperlipidemia)
Primary Hypercholesterolemia: Clinical Classification • Elevated LDL cholesterol (>160 mg/dl; 1/4 of all American Adults) • - Familial Hypercholesterolemia (1/500) • - Familial Combined Hyperlipidemia (1/100) • - Polygenic Hypercholesterolemia (1/4)
Dietary Hyperlipidemia VLDL remnants apoB-100 VLDL Apo E Caloric intake Overproduction of VLDL TG Apo C X X Reduced activity of LDL receptors ( Saturated fat and cholesterol In the diet) LDL LDL Increased conversion to LDL Other sites
Reverse cholesterol transport CE FC Mature HDL Bile Macrophage Nascent HDL A-I A-I FC CE LCAT FC CE ABCA1 Liver
Reverse cholesterol transport : Role of CETP in HDL Metabolism Mature HDL Bile Macrophage Nascent HDL A-I A-I FC CE CE LCAT FC FC CE ABCA1 SR-BI SRA CETP Liver CE LDLR Oxidation TG CE B VLDL/LDL CETP = cholesteryl ester transfer protein
Secondary Causes of Low HDL-C Smoking Obesity (visceral fat) Sedentary Lifestyle High carbohydrate or very-low-fat diet Hypertriglyceridemia (from any cause) Drugs Beta-blockers Androgenic steroids Androgenic progestins
Cholesterol disorders associated with premature CAD Familial Hypercholesterolemia Low HDL Nephrotic Syndrome Lp(a) [ not ApoA]. Triglyceride Disorders associated with premature CAD (+) premature CAD (-) premature CAD Familial Combined HLD Familial HTG Remnant Removal Dz Familial Chylomicronemia Central Obesity (metabolic syndrome) Estrogen Diabetes Alcohol Nephrotic syndrome/Uremia/dialysis Bile Acid Resins Hypothyroidism High Carbohydrate diet Cushing’s syndrome
New Concepts in Atherosclerosis Risk: Triglycerides, Small Dense LDL and the Metabolic Syndrome
BP Atherogenic Dyslipidemia HDL Metabolic Syndrome Procoagulant State Insulin Resistance
Hypertension Thrombosis Pro Coagulant State TG HDL VLDL IDL Cigarette Smoking LDL Diabetes Atherosclerosis CHD
Metabolic Consequences of Hypertriglyceridemia Small, dense LDL Chylomicron remnants HYPERTRIGLYCERIDEMIA VLDL remnants HDL IDL
Insulin Resistance and Dyslipidemia TG Apo B VLDL HDL VLDL SD LDL v Fat Cells Liver FFA CE (CETP) TG IR Apo A-I CE (CETP) TG Kidney LDL (lipoprotein or hepatic lipase) Insulin
Significance of Small, Dense LDL Low cholesterol content of LDL particles particle number for given LDL-C level Associated with levels of TG variable LDL-C, and levels of HDL2 Marker for common genetic trait associated with risk of coronary disease (LDL subclass pattern B) Possible mechanisms of atherogenicity greater arterial uptake uptake by macrophages oxidation susceptibility Feingold KR et al. Arterioscler Thromb. 1992;12:1496-1502. Lamarche B et al. Circulation. 1997;95:69-75.
C Atherogenic Particles E E B B B Small VLDL Remnant LDL IDL
Atherogenic Cholesterol VLDL + IDL + LDL = Total Cholesterol - HDL = non HDL cholesterol
Calculating LDL Cholesterol • LDL-C = TC – HDLC – TG/5 • Invalid when TG > 400 mg/dl • Underestimates “atherogenic cholesterol” • when TG >200 mg/dl • nonHDL-C = TC - HDLC
Non-HDL Cholesterol Predictive of CV Events Rates in Prospective Clinical Trials Useful when triglycerides > 200 mg/dl Allows use of NCEP LDL guidelines (+ 30 mg/dl) Flexible - Allows use of non fasting samples to assess lipid treatment goals
ATP III: The Metabolic Syndrome* *Diagnosis is established when 3 of these risk factors are present. †Abdominal obesity is more highly correlated with metabolic risk factors than is BMI. ‡Some men develop metabolic risk factors when circumference is only marginally increased. Expert Panel on Detection, Evaluation, and Treatment ofHigh Blood Cholesterol in Adults. JAMA. 2001;285:2486-2497.
ATP III: New Features of Guidelines—Focus on Multiple Risk Factors Persons with diabetes without CHD raised to level of CHD risk equivalent Framingham 10-year absolute CHD risk projections used to identify certain patients with 2 risk factors for more intensive treatment Persons with multiple metabolic risk factors (the metabolic syndrome) identified as candidates for intensified therapeutic lifestyle changes (TLC) Expert Panel on Detection, Evaluation, and Treatment ofHigh Blood Cholesterol in Adults. JAMA. 2001;285:2486-2497.