Understanding Dementia: Types, Symptoms, Assessment, and Management
This comprehensive overview discusses dementia, including its definitions, types, and symptoms. It defines dementia as cognitive deficits that interfere with social or occupational functioning. Key forms of dementia like Alzheimer's disease, vascular dementia, and frontotemporal dementia are examined alongside their diagnosis and progression. The course of Alzheimer’s, highlighting early memory impairment and late-stage behavioral disturbances, is detailed. Assessment techniques for cognitive function, activities of daily living, and factors influencing risk are also explored.

Understanding Dementia: Types, Symptoms, Assessment, and Management
E N D
Presentation Transcript
Who are you again? No ifs, ands, or, buts.. Treatment Prevention Definitions Assessment $100 $100 $100 $100 $100 $200 $200 $200 $200 $200 $300 $300 $300 $300 $300 $400 $400 $400 $400 $400 $500 $500 $500 $500 $500
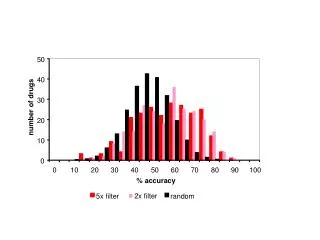
What is the definition of dementia? Acquired cognitivedeficits sufficient to interfere with social or occupational functioning in person without depression or clouding of consciousness Alzheimer’s disease 60% Mixed 20% Lewy body 10% Vascular dementia 5% Fronto-temporal 4% CJD <1%
What is vascular dementia? • patchy loss of neurons in areas of infarcts (multi-infarct, lacunar, periventricular) • cognitive changes depend on area of infarct • recall improves with cuing, more aware of memory problem • Diagnosis: • dementia • vascular component – by hx, px or imaging • temporal relationship between • abrupt onset • stepwise decline • impaired executive function • gait disorder • emotional lability • clinical/neuroimaging evidence of cerebrovascular disease
What is fronto-temporal dementia? • EtOH, COPD, Picks, CBGD, Huntingtons • memory relatively well-preserved • core diagnosis (in italics): • insidious onset • slow progression • behavioural changes – loss of social awareness (disordered social conduct), disinhibition, emotional blunting, mental rigidity, inflexibility, hyperorality, perseveration, distractibility, loss of insight, declining hygiene, character change • language changes with reduction in verbal output
DAILY DOUBLE Name 1 test that can be used to check frontal lobe function word list - name as many 4-legged animals as can in 1 min trails - trail A (A-B-C-D..), trail B (A-1-B-2-C-3..) similarities/differences - apple/orange, vinegar/salt
What is Lewy body dementia? • neuronal loss in limbic, substantia nigra, autonomic system • memory loss + motor changes + hallucinations early • like an AD + PD • 2 of (probable DLB) or 1 (possible) of following: • .fluctuating sx, with variation in alertness and attention • .recurrent visualhallucinations, typically well-formed and detailed • .spontaneous extrapyramidal signs/motor features of Parkinsonism • Features supportive for diagnosis are: • repeated falls • hypersensitivity to neuroleptics • delusions • nonvisualhallucinations • syncope/transient LOC • drug-unresponsive depression • REM sleep – acting out, vivid violent dreams
What is Alzheimer’s disease? DAILY DOUBLE • DSM IV criteria for AD • The development of multiple cognitive deficits that is manifested by BOTH of: • memory deterioration • >=1 of aphasia (language) • agnosia (objects) • apraxia (motor activities) • executive function impairment (planning, organising, sequencing) • is a significant decline compared to previous fn • causes significant impairment in social/occupational function • gradual onset, continuing decline NOT due to cerebrovascular dz, Huntington’s dz, Parkinson’s dz, systemic conditions know to cause dementia (hypothyroidism, vit B12 deficiency, folic acid deficiency, neurosyphilis, HIV infection), substance-induced conditions, delirium, major depressive disorder, schizophrenia
What is the course of Alzheimer’s disease? Early memory impairment – recent>remote Middle/Late behavioural disturbances – agitation, aggression, combativeness, shouting, disinhibition psychotic sx – paranoia, delusions, hallucinations wandering behaviour gait, motor disturbances, incontinence
What are the most important elements of the HPI? Memory deterioration - recent, remote Aphasia - probs understanding language, names of things, reading/writing Apraxia - inability to carry out goal-oriented motorfunctions e.g. getting dressed in correct order Agnosia - inability to recognise people and objects Executive function - ability to anticipate, select, initiate an action, plan and organise a procedure e.g. financial planning Depression Delusions Hallucinations Personality changes Apathy Agitation
What are important questions in PMH, FH, & SH? PMH Systemic diseases, ca, neurological, psychiatric, thyroid disorders HTN, a fib, Head injury EtOHism, FH Dementia, AD (2-4 x increased risk if 1st degree relative), Huntington's dz SH EtOH, smoking, substance abuse Occupational exposures Level of education
What medication hx is it important to elicit? • narcotics • anticholinergics • benzodiazepines • psychotropics • OTC, herbal
How can you assess functional status? ADL “DEATH” Dressing Eating Ambulating Toileting Hygiene IADL “SHAFT” Shopping Housekeeping Accounting Food preparation Transportation • FAQ (functional activities questionnaire) • bill paying • assembling records relating to business affairs • shopping alone • playing a game of skill • performing a task involving multiple steps (writing letter, stamping envelope, placing in mailbox) • preparing a balanced meal • being aware of current events • understanding and discussing TV, book etc • remembering and keeping appointments • driving, arranging to take bus, walking to familar places
What is the prevalence of comorbid depression? prevalence in pts with AD is 6-20% • weight & sleep changes • sadness • crying • suicidal statements • excessive guilt
What parts of physical exam are important in dementia? • VS incl postural • vision • hearing • CNs • motor, sensory function esp localising sx, Parkinsonism, stroke • reflexes
What’s normal anymore?MMSE ‘NORMALS’ LIMITATIONS CORRECT FOR EDUCATION, AGE
How is clock drawing scored? • Give 1 point for each of the following: • all 12 correct numbers, • hands in correct position, • closed circle, • numbers in correct position • <4 needs further evaluation
FREEBIE! $400 FREE!
How are DSM IV criteria tested? memory aphasia apraxia agnosia executive fn hold pt repeats 6 or 7 digits forward, 3 or 4 digits backwards recent pt recounts simple short story, 4-5 sentences remote significant national/international events language production -verbal name body parts or objects in room - written writes 1 sentence describing what is wearing comprehension - verbal simple command e.g. walk over to window - written simple written request pt demonstrates e.g. how to use toothbrush coins give pt instructions to plan, initiate and sequence a task
Draw a clock! 4 points = $400!!
What bloodwork is recommended by CMA guidelines? CBC, lytes, Ca2+ TSH, glucose That’s it!!
Name 3 additional tests to consider Optional additional tests: lipids, BUN/creatinine ESR, serum cortisol ammonia, LFTs, B12/folate, water soluble vitamins drug levels, heavy metal levels VDRL, HIV blood gas carotid dopplers CXR, ECG, EEG, LP, mammography
Name 4 indications for CT head in dementia • Indications for CT head: • age <60 y.o. • rapid decline (months) • short duration (<2 yrs) • recent headtrauma • new localising sx (Babinski, hemiparesis) • unexplained neuro finding (HA, sz) • urinary incontinence + gait disturbance early on (NPH) • incontinence • anticoagulation, bleeding dz • cancer history • atypical presentation • gait disturbance
What are 2 non-pharmacological therapies for dementia? • verbal/physical prompts with positive reinforcement • memory training • read newspapers, watch educational shows on TV • reminders about content of conversations
Who do we screen? No evidence to recommend screening for cognitive impairment in absence of sx Memory complaints should be followed up
What is the pharmacological treatment of dementia? Acetylcholinesterase inhibitors (AChE) • donepezil (Aricept) AchE 2 point improvement MMSE after 3 mos • rivastigmine (Exelon) AchE + butyrcholinesterase inhib • galantamine (Reminyl) AchE + nicotinic receptor inhib Indicated for: AD MMSE 10-26 Lewy body mixed
Acetylcholinesterase Inhibitors DonepezilRivastigmineGalantamine Indication AD AD, Lewy body AD, mixed Metabolism hepatic + renal hepatic + renal Dose interval daily in AM BID BID Initial dose 5 mg 1.5 mg 4 mg Min titration interval 4 weeks 4 weeks 4 weeks Lowest therapeutic 5 mg daily 3 mg BID 4 mg BID Target dose 10 mg daily 4.5 – 6 mg BID 8 mg BID Max dose 10 mg 6 mg BID 12 mg BID ODB coverage covered LU – 354 (1st 3 mos) LU – 355 (after 3 mos)
Give me 1 tip on starting therapy... Start low, go slow! Reassess in 4 weeks to increase dose, reassess at 2 weeks if necessary to assess tolerability Warn pt of common side-effects: nausea, anorexia, diarrhoea, dizziness, agitation Repeat MMSE at 3 mos – need improvement or stabilization. Expected decline in MMSE on treatment is <3 points/year
Name 1 treatment for behavioural problems At some point during illness, 90% pts have behavioural problems. Review possible triggers (illness, pain, mealtimes, loneliness) Non-pharmacological treatment: familiar routines sensory stimulation – auditory, visual, tactile low lighting levels, music, simulated nature sounds may be calming exercise program with outdoor daily walking if possible (decreases wandering, agitation) pet therapy Pharmacological treatment: low dose neuroleptic drugs (risperidone, olanzepine, quetiapine).e.g. risperidone 1mg daily shown to be effective and well-tolerated SSRI trazodone (esp for sleep disturbances) CAUTION with benzodiazepines – use only in low doses and PRN AVOID neuroleptics with marked anticholinergic effects e.g. chlorpromazine
Name 2 interventions for the prevention of dementia treat vascular risk factors: antihypertensives, statins (hypercholesterolemia), anticoagulants (a fib), smoking cessation, DM control, antiplatelets, carotid endarterectomy (stroke prevention) correction of metabolic disturbances improved basic education decrease head injury incidence ?post-menopausal HRT (case control, cohort studies) ?NSAIDs ginkgo biloba – no evidence for or against Vit E 2000 IU daily – no evidence for or against
When do you refer? Give me 1 instance.... • early behavioural changes • delusions • fluctuating course • early motor changes • atypical pattern • uncertainty about diagnosis after initial assessment and follow-up • request by family/pt for another opinion • presence of significant depression esp if refractory to tx • treatment problems or failure • need for additional help in management • when geneticcounselling is indicated • when research studies into diagnosis and treatment are being carried out