Download
1 / 16
160 likes | 616 Vues
Groundwater Arsenic Concentrations and Cancer Incidence Rates: A Regional Comparison in Oregon. Harmony Fleming, MS Anna K Harding, PhD Department of Public Health Oregon State University. Background:.

E N D
Groundwater Arsenic Concentrations and Cancer Incidence Rates: A Regional Comparison in Oregon Harmony Fleming, MS Anna K Harding, PhD Department of Public Health Oregon State University
Background: • Chronic exposure to arsenic in drinking water has been linked to both carcinogenic and non-carcinogenic health effects in humans. • Health effects associated with inorganic exposure include: • tumors of the bladder, kidney, liver, and lung; blood vessel damage; • reproductive and developmental effects; neurological effects; peripheral vascular and cardiovascular disease; diabetes mellitus; and • dermal effects such spotted melanosis, leucomelanosis and keratosis and basal cell cancer of the skin.
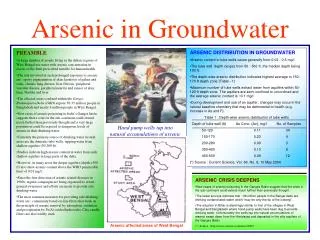
Background: • Primary exposure route is ingestion from drinking water due to contamination in groundwater from dissolution of natural mineral deposits, industrial effluent and drainage problems. • Current MCL for public water systems is 10 ppb (2006) which was reduced from 50 ppb • Considerable proportion (25%) of Pacific NW population relies on private wells for domestic water supply—no enforceable MCL • Known “hot spots” for higher arsenic levels in at least two geographic areas in Oregon—Willamette Valley and southeastern Oregon • Interest in investigating if the population drawing groundwater from these areas at higher risk of cancer
Study Objectives: • Determine if there is a spatial relationship between arsenic concentrations in the Willamette Valley and Southeast Oregon and incidence rates of bladder, liver, lung, and kidney cancers • Contribute to the Centers for Disease Control and Prevention’s development of the Environmental Public Health Tracking network by using secondary data to investigate linkages of arsenic in groundwater and associated health effects • Serve as an exploratory tool for identifying a public health concern that can be followed up with comprehensive analytical studies of the region
Data sets used for analyses: • Oregon State Cancer Registry; bladder, liver, lung & kidney cancer data for the year 2000 • Oregon Department of Human Services Drinking Water Program; community water system arsenic data • U.S. Geological Survey National Water Inventory System; groundwater arsenic data • U.S. Census Bureau; population data from 2000 Census
Limitations of Secondary Data: • Data sets used to answer research questions had not been collected for the purpose of identifying causal relationships between arsenic concentrations and cancer incidence. • Arsenic exposure is inferred by the presence of arsenic in groundwater that is known to supply domestic water supplies. • An implied surrogate exposure may not accurately represent the actual exposure of the population. • Cancer cases located in rural areas not always geocodable by state cancer registry (e.g. only 58% of cases in Harney County were included)
Methods: • Data were analyzed both statistically and spatially using SAS, Excel and ArcGIS. • The three independent variables; arsenic concentration, age and sex were grouped into intervals for the analyses:
Statistical Methods: • Use Chi-square to compare the observed cancer cases (for each cancer type) to the expected cancer case count for the five census tract groups for both genders. • Poisson regression was used to attempt to determine if significant differences of observed cancer occurrence exist within the three categories; age, gender and census tract quintile groups. Spatial Display: • A spatial representation of the data was created with ArcGIS by linking the arsenic concentration and census tract attributes of the study area.
The Maps show that: • Arsenic in groundwater is widely distributed throughout the regions. • Arsenic concentration levels vary greatly between census tracts located in close proximity • Aggregated values of arsenic are the mean of all arsenic samples within a census tract from both the USGS data and DWP community water system data. • Aggregated concentration values in some cases were considerably lower than the highest sample value. Obvious limitation to accurately estimating arsenic concentrations in groundwater.
Results: Table 1. Chi-square Values for Age & Sex-specific Incidence Rates: Differencesbetween Observed & Expected Cancer Counts Table 1. Chi-square Values for Age & Sex-specific Incidence Rates: Differences between Observed & Expected Cancer Counts Table 1. Chi-square Values for Age & Sex-specific Incidence Rates: Differences between Observed & Expected Cancer Counts Table 1. Chi-square Values for Age & Sex-specific Incidence Rates: Differences between Observed & Expected Cancer Counts Table 1. Chi-square Values for Age & Sex-specific Incidence Rates: Differences between Observed & Expected Cancer Counts
Results: The Chi-square values among all the individual cancer types resulted in non-significant values suggesting arsenic concentration did not contribute to differences between the observed and expected cancer counts within the study area.
Results: Table 2. Risk Ratios and Confidence Intervals for Arsenic Concentration Table 2. Risk Ratios and Confidence Intervals for Arsenic Concentration Table 2. Risk Ratios and Confidence Intervals for Arsenic Concentration
Results: The individual regression analysis of each cancer type and the combined group resulted in non-significant results indicating that higher arsenic concentrations did not increase the incidence rate of the four cancers (bladder, kidney, liver and lung) after adjusting for age and sex.
Conclusions: • The use of geographic information systems (GIS) provides the platform to analyze health effects in proximity to environmental hazards, which is important for public health intervention & prevention activities—great potential for EH studies. • Spatial study of groundwater arsenic and associated health outcomes had not been previously done in Oregon—secondary data had definite limitations • The results contradicted numerous epidemiologic studies that have found a positive association between arsenic ingestion and increased cancer incidence.
Conclusions: • The statistical and spatial analytical problems inherent to substituting individual-level data with aggregate data may not have identified the actual risk to individuals. • Surrogate exposure levels are not the optimal measurement for analysis but when used with a GIS, they may give a better understanding of associations between environmental contaminants and disease rates. • Majority of census tracts fall into Quintiles 1 and 2, which are below MCL • Missing cases in rural areas might contribute to underestimation of cancer incidence rates in these census tracts