Download
1 / 12
130 likes | 227 Vues
This informative content explains the role of various forms of calcium in blood, the influence of acid-base balance on ionized Ca2+ concentration, absorption and secretion processes, as well as the regulation of Parathyroid Hormone (PTH) and Calcitonin in calcium homeostasis. ###

E N D
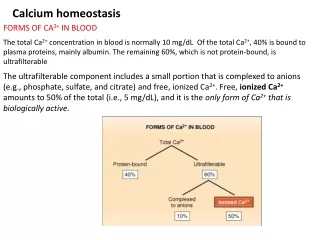
Calcium homeostasis FORMS OF CA2+ IN BLOOD The total Ca2+ concentration in blood is normally 10 mg/dL Of the total Ca2+, 40% is bound to plasma proteins, mainly albumin. The remaining 60%, which is not protein-bound, is ultrafilterable The ultrafilterable component includes a small portion that is complexed to anions (e.g., phosphate, sulfate, and citrate) and free, ionized Ca2+. Free, ionized Ca2+ amounts to 50% of the total (i.e., 5 mg/dL), and it is the only form of Ca2+ that is biologically active.
Acid-base abnormalities alter the ionized Ca2+ concentration by changing the fraction of Ca2+ bound to plasma albumin . Albumin has negatively charged sites, which can bind either H+ ions or Ca2+ ions. In acidemia, there is an excess of H+ in blood; thus more H+ binds to albumin, leaving fewer sites for Ca2+ to bind. In acidemia, the free ionized Ca2+ concentration increases because less Ca2+ is bound to albumin. In alkalemia, there is a deficit of H+ in blood, and less H+ will be bound to albumin, leaving more sites for Ca2+ to bind.
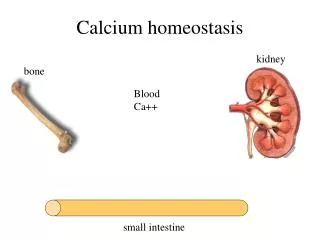
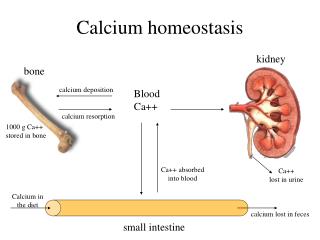
the person ingests 1000 mg of elemental Ca2+ daily, approximately 350 mg is absorbed from the gastrointestinal tract, a process that is stimulated by the active form of vitamin D, 1,25-dihydroxycholecalciferol. However, about 150 mg/day is secreted into the gastrointestinal tract in salivary, pancreatic, and intestinal fluids. Thus, netabsorption of Ca2+ is 200 mg/day (350 mg -150 mg), and the remaining 800 mg/day (of the 1000 mg ingested) is excreted in feces. The absorbed Ca2+ enters the Ca2+ pool in ECF. There are four parathyroid glands in humans, located in the neck under the thyroid gland. The chief cells of the parathyroid glands synthesize and secrete PTH, a single-chain polypeptide with 84 amino acids .
Regulation of PTH Secretion PTH secretion is regulated by the plasma Ca2+ concentration. , when the total Ca2+ concentration is in the normal range (i.e., 10 mg/dL) or higher, PTH is secreted at a low (basal) level. However, when the plasma Ca2+ concentration decreases to less than 10 mg/dL, PTH secretion is stimulated, reaching maximal rates when the Ca2+ concentration is 7.5 mg/dL. Although it is actually the ionized Ca2+ concentration that regulates secretion by the parathyroid glands. The response of the parathyroid glands to a decrease in ionized Ca2+ concentration is remarkably prompt, occurring within seconds. Furthermore, the faster the ionized Ca2+ falls, the greater the PTH secretory response
The actions of PTH on bone, kidney, and intestine are described as follows: Bone. PTH has several actions on bone, some direct and some indirect. In bone, PTH receptors are located on osteoblasts but not on osteoclasts. Initially and briefly, PTH causes an increase in bone formation by a direct action on osteoblasts. (This brief action is the basis for the usefulness of intermittent PTH administration in the treatment of osteoporosis.) Kidney. PTH has two actions on the kidney. (1) PTH inhibits phosphate reabsorption by inhibiting Na+-phosphate cotransport in the proximal convoluted tubule. (2) PTH stimulates Ca2+ reabsorption. Small intestine. PTH does not have direct actions on the small intestine, although indirectly it stimulates intestinal Ca2+ absorption via activation of vitamin D. PTH stimulates renal 1α-hydroxylase, the enzyme that converts 25-hydroxycholecalciferol to the active form, 1,25-dihydroxycholecalciferol. In turn, 1,25-dihydroxycholecalciferol stimulates intestinal Ca2+ absorption
Figure 9-34 Ca2+ homeostasis in an adult eating 1000 mg/day of elemental Ca2+. Hormonal effects on Ca2+ absorption from the gastrointestinal tract, bone remodeling, and Ca2+ reabsorption in the kidney are shown. PTH, Parathyroid hormone
Regulation of PTH secretion and PTH actions on bone, kidney, and intestine. cAMP, Cyclic adenosine monophosphate; PTH, parathyroid hormone
CALCITONIN Calcitonin is a straight-chain peptide with 32 amino acids . It is synthesized and secreted by the parafollicular or C ("C" for calcitonin) cells of the thyroid gland. The calcitonin gene directs the synthesis of preprocalcitonin and a signal peptide is cleaved to yield procalcitonin; other peptide sequences are then removed, and the final hormone, calcitonin, is stored in secretory granules for subsequent release The major stimulus for calcitonin secretion is increased plasma Ca2+ concentration (contrast this with the stimulus for PTH secretion, decreased plasma Ca2+ concentration). The major action of calcitonin is to inhibit osteoclastic bone resorption, which decreases the plasma Ca2+ concentration.
Vitamin D Vitamin D, in conjunction with PTH, is the second major regulatory hormone for Ca2+ and phosphate metabolism. The roles of PTH and vitamin D can be distinguished as follows: The role of PTH is to maintain the plasma Ca2+ concentration, and its actions are coordinated to increase the ionized Ca2+ concentration toward normal. Vitamin D (cholecalciferol) is provided in the diet and is produced in the skin from cholesterol. Vitamin D has formal "hormone" status because cholecalciferol itself is inactive and must be successively hydroxylated to an active metabolite. Hydroxylation of cholecalciferol is regulated by negative feedback mechanisms
Actions of Vitamin D The overall role of vitamin D (1,25-dihydroxycholecalciferol) is to increase the plasma concentrations of both Ca2+ and phosphate and to increase the Ca2+ × phosphate product to promote mineralization of new bone. To increase plasma Ca2+ and phosphate concentrations, vitamin D has coordinated actions on intestine, kidney, and bone. Because 1,25-dihydroxycholecalciferol is a steroid hormone, its mechanism of action involves stimulation of gene transcription and synthesis of new proteins, which have the following physiologic actions
Pathophysiology of Vitamin D In children, vitamin D deficiency causes rickets, a condition in which insufficient amounts of Ca2+ and phosphate are available to mineralize the growing bones. Rickets is characterized by growth failure and skeletal deformities. This condition is rare in areas of the world where vitamin D is supplemented and when there is adequate exposure to sunlight. Vitamin D resistance occurs when the kidney is unable to produce the active metabolite, 1,25-dihydroxycholecalciferol. This condition is called "resistant," because no matter how much vitamin D is supplemented in the diet, it will be inactive because the C1 hydroxylation step in the kidney is absent or is inhibited. Vitamin D resistance can be caused by the congenital absence of 1α-hydroxylase or, more commonly, by chronic renal failure. Chronic renal failure is associated with a constellation of bone abnormalities, including osteomalacia, a consequence of the inability of the diseased renal tissue to produce 1,25-dihydroxycholecalciferol, the active form of vitamin D