Download

1 / 28
330 likes | 693 Vues
Calcium Homeostasis I. Dr. Sumbul Fatma. Introduction. Calcium has a lot of cellular and tissue effects involving contractile machinery, structural roles, enzymatic reactions etc All these effects depend upon the blood calcium to be within normal limits. Calcium Distribution.

E N D
Calcium Homeostasis I Dr. Sumbul Fatma
Introduction • Calcium has a lot of cellular and tissue effects involving contractile machinery, structural roles, enzymatic reactions etc • All these effects depend upon the blood calcium to be within normal limits
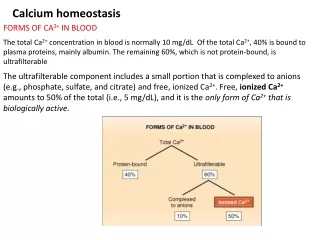
Calcium Distribution • 99 % is part of bone and 1% is present in blood and ECF • Calcium distribution in blood – - 45% circulates as free calcium ions referred to as ionized calcium - 40% is bound to protein (albumin) - 15% is bound to anions such as bicarbonate, citrate, phosphate, and lactate (conc. of these anions can change dramatically during surgery or critical care and therefore, ionized calcium cannot be reliably calculated from total calcium measurements)
Ionized calcium • It is important to maintain ionized calcium because decreased ionized calcium - impairs myocardial function, and can also cause - neuromuscular irritability, which may become apparent as irregular muscle spasms, called tetany
Samples for calcium measurement Sample- Blood and Urine • Total Calcium- Serum or lithium heparin plasma • Ionized Calcium - anaerobic collection - heparinized whole blood preferred - serum from sealed evacuated blood collection tubes
Heparin for ionized calcium • No liquid heparin should be used as most heparin anticoagulants (sodium/lithium) partially bind to calcium and lower ionized calcium concentrations. e.g. 25 IU/mL heparin decreases calcium concentration by 3% • Dry heparin products titrated with small amounts of calcium or zinc ions or with small amounts of heparin in an inert puff that essentially eliminates the interference by calcium should be used
Urine for calcium analysis • Urine - Accurately timed collection - Urine should be acidified with 6M HCl with ~1ml HCl per 100mL of urine
Total Calcium determination • Dyes are used that form a complex with calcium. Prior to dye binding the sample is acidified so that calcium is released from its protein carriers and complexes e.g. ortho-cresolphthalein complexone (CPC) or arsenzo III dye • Atomic Absorption Spectrophotometer (AAS) is used as the reference method for whole blood analysis
Ionized Calcium determination • Commercial analyzers use Ion selective electrodes (ISEs) for calcium measurement. These systems may use membranes impregnated with special molecules that selectively but reversibly bind calcium ions. As calcium ions bind to these membranes an electric potential develops across the membrane that is proportional to the ionized calcium concentration
Total Calcium versus ionized calcium During surgery, the patients may receive large amounts of citrate, bicarbonate, calcium salts or fluids, the greatest discrepancies between total and ionized calcium concentration may be seen during these times. Consequently, ionized calcium measurements are the calcium measurements of greater clinical value
Regulation of calcium Three hormones regulate serum calcium by altering their secretion rate in response to changes in ionized calcium 1. Parathyroid hormone (PTH) 2. Vitamin D, and 3. Calcitonin
Parathyroid hormone (PTH) • A decrease in ionized calcium leads to increase in PTH secretion and it is decreased with an increase in calcium concentration • PTH exerts three major effects on both bone and kidney 1. In bone, PTH activates bone resorption, a process in which activated osteoclasts breakdown bone and subsequently release calcium into the extracellular fluid 2. In Kidneys, PTH conserves calcium by increasing tubular reabsorption of calcium ions 3. PTH also stimulates renal production of active Vitamin D
Vitamin D synthesis • Vitamin D in reality is a hormone and is a metabolic product of the cholesterol biosynthetic pathway • Vitamin D3, a cholecalciferolis synthesized de novo by the exposure of skinto sunlight that converts 7-dehydrocholesterol to vit D3 • Vitamin D3 is then converted in liver, to 25-hydroxycholecalciferol (25-OH- D3) by the enzyme 25-hydroxylase - still an inactive form • 25-OH- D3 is the blood test used to assess adequacy of vitD stores in the body • In the kidney, renal 1 α-hydroxylase hydrolyses 25-OH- D3 to form 1,25-dihydroxycholecalciferol (1,25-[OH]2- D3) – the biologically active form (PTH stimulates this enzyme)
Vitamin D from diet • Vitamin D is relatively rare in most typical foods • The only common dietary source of vitamin D are multivitamins , supplements and vitamin D fortified milk • Cod liver oil is also a source of vitamin D
Vitamin D regulation • Vitamin D receptor (VDR) is a nuclear receptor that carries out physiologic regulation by directing transcription of specific vitamin D responsive genes
Vitamin D regulation • Stimulates osteoblasts to release cytokines to influence osteoclasts to mobilize bone calcium- bone resorption • In small intestinal epithelial cells, vitamin D upregulates expression of numerous genes that stimulate transepithelial calcium transport from the intestinal lumen into the blood. The site of maximal absorption is duodenum • Blood calcium feeds back to parathyroid tissue and affects synthesis and secretion of PTH • Also, vitamin D-VDR complex down-regulates PTH expression
Calcitonin • It is not secreted during normal regulation of the ionized calcium in blood • Increased concentration of calcium in blood leads to secretion of calcitonin from the medullary cells of thyroid gland • It lowers calcium by inhibiting the action of PTH and vitamin D
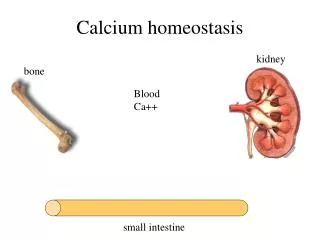
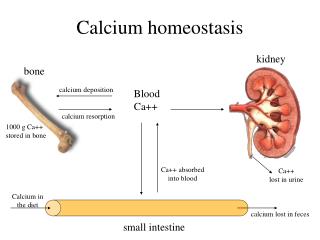
Organs involved in calcium homeostasis • Calcium is in constant flux entering and leaving the blood pool • The principal organs involved in this flux are - small intestine - bone - kidney
Gastrointestinal tract • All calcium that enters the body arrives via GI absorption • Normal vitamin D availability is required for optimal calcium absorption (doubles the calcium absorption) • Dietary phosphate can bind dietary calcium in the intestinal lumen and precipitate as insoluble calcium phosphate preventing the absorption of both • A diet high in phosphate (e.g. junk food diet or high consumption of dark soda pops) tend to inhibit calcium absorption
Renal • The real net loss of calcium from the body occurs via the kidneys in urine • Kidneys reabsorb the calcium in the tubules and also excrete the calcium in urine depending upon the total filtered load
Bone • Chief reservoir of calcium in the body • It can serve to remove calcium from the blood to be stored in bone and release calcium stored in bone to the blood
Summary • Calcium homeostasis is a complex balance between into blood and out of blood factors , which reflects integrated endocrine and organ physiology • Any disturbance in this balance results in alterations in calcium metabolism that can lead to various medical conditions
References • Clinical Chemistry by Bishop, Fody and Schoeff Chapters- 13 and 21