Download
1 / 3
40 likes | 128 Vues
Rates for Dental Hygienists / Dental Assistants start at $99 for $1,000,000 / $3,000,000 of Professional Liability coverage, available in all 50 states.

E N D
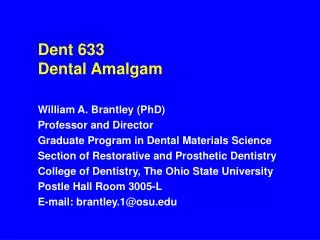
Dental Hygienist / Dental Assistant Professional Liability Application 1. First Name Middle Initial Last Name Street Address Suite / Bldg. Number City State Zip Code Telephone # e-Mail Address Professional License # 2. Please indicate your profession : Dental Hygienist Dental Assistant 3. Indicate your employment : Employed Self-Employed under Supervision Self-Employed not under Supervision 4. Desired effective date : 5. Please indicate Limits of Liability desired: $100,000 / $300,000 $250,000 / $500,000 $250,000 / $750,000 $500,000 / $500,000 $500,000 / $1,500,000 $1,000,000 / $1,000,000 $1,000,000 / $2,000,000 $1,000,000 / $3,000,000 6. Deductibles : $0 $1,000 $2,500 $5,000 $7,500 $10,000 $25,000 Greater than $25,000 7. Desired retroactive date : 8. If student please provide the anticipated graduation date : 9. List of Professional Association of which you are a member : 10. Have you ever been the subject of a reprimand or disciplinary action or refused employment or admission to a professional society or had your professional privileges suspended by any court or administrative agency or ever been the subject of any ethics investigation at a local, state or national level? No Yes If yes, please explain below. NDPG APP 01/11 Page 1 of 3
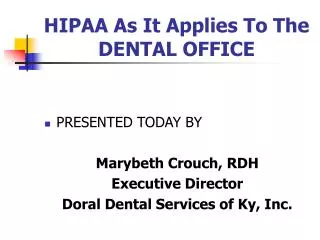
Dental Hygienist / Dental Assistant Professional Liability Application 11. Has any insurance ever been cancelled or non-renewed? No Yes If yes, please explain 12. Has any malpractice claim or suit ever been brought against you? No Yes If yes, please explain 13. Please list your prior professional liability insurance, if any. Insurance Carrier Policy # Limits Effective Date I understand and agree this Application and any and all supplements attached hereto may be made a part of any policy issued, and any such policy will be issued in reliance upon the representation made herein. I further understand and agree that failure to provide a true and accurate response to the foregoing questions may, at the option of the Company, result in the voiding of insurance issued in reliance on this Application and/or denial of claims under any policy issued. I authorize and consent to investigations of information bearing upon moral character, professional reputation and fitness to engage in the activities of my business including authorization to every person or entity, public or private, to release to the company providing insurance coverage and The National Dental Purchasing Group any documents, records or other information bearing upon the foregoing. NDPG APP 01/11 Page 2 of 3
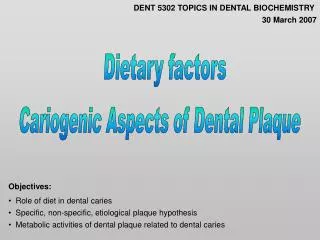
Dental Hygienist / Dental Assistant Professional Liability Application I understand and agree these investigations shall not be confined to information submitted in this application, but shall include any other sources of information deemed relevant by the Company as may be authorized by law. Applicant and all owners, employees, and contractors are licensed or duly authorized in all states or jurisdictions where professional services are provided. Applicant warrants the truth of all answers to the above questions, and that applicant has not withheld any information which is calculated to influence the judgment of the insurance company in considering this application. IMPORT ANT : T HIS APPLICAT ION MUS T BE S IGNED BY T HE APPLICANT . S IGNING T HIS FORM DOES NOT BIND T HE COMPANY T O COMPLET E T HE INS URANCE. Applicant Name Date NDPG APP 01/11 Page 3 of 3