Duloxetine for Relapse Prevention in Generalized Anxiety Disorder: A Double-Blind Study
This study evaluates the efficacy of duloxetine (60-120 mg once daily) for preventing relapse in adults with generalized anxiety disorder (GAD). Conducted over 52 weeks, it involved an initial open-label phase followed by a double-blind placebo-controlled phase with 887 patients. Results indicate that duloxetine significantly reduced relapse rates compared to placebo, with 13.7% of duloxetine-treated patients relapsing versus 41.8% on placebo. The treatment was well-tolerated, with a lower incidence of discontinuations due to adverse events.


Duloxetine for Relapse Prevention in Generalized Anxiety Disorder: A Double-Blind Study
E N D
Presentation Transcript
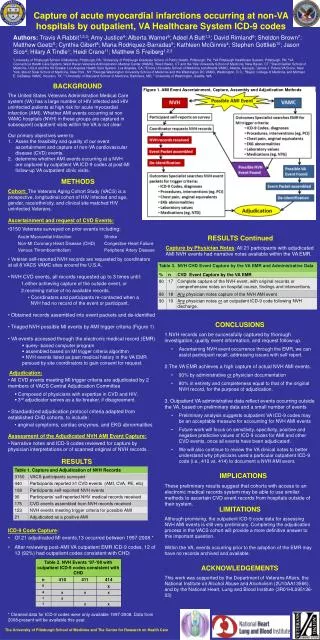
* Open-Label Acute Phase Double-Blind Phase Screening DLX 120 mg QD DLX 60-120 mg QD DLX 90 mg QD Taper All Patients DLX 60 mg QD -3 to -30 days DLX 30 mg QD Placebo 55 0 1 5 8 26 52 Weeks Randomization of Responders DLX = Duloxetine Duloxetine 60 to 120 mg Once Daily for the Prevention of Relapse in Adults with Generalized Anxiety Disorder: A Double-blind Placebo-controlled Trial Sponsored by Dr. Jonathan Davidson Jonathan RT Davidson MD1, Hans-Ulrich Wittchen PhD2, Pierre-Michel Llorca MD3, Janelle Erickson PhD4*, Michael J Detke MD, PhD.4,5,6, Susan G Ball PhD4,6, James M Russell MD4 1 Duke University Medical Center, Durham, NC; 2 Technische Universitat Dresden, Dresden, Germany; 3 C.H.U. Clermont-Ferrand, France; 4 Lilly Research Laboratories, Indianapolis, IN; 5 McLean Hospital/Harvard Medical School, Boston, MA; 6 Indiana University School of Medicine, Indianapolis, IN; * Current affiliation Orexigen Therapeutics, San Diego, CA Key Inclusion Criteria ABSTRACT Table 2. Mean Changes from Double-blind Randomization to Study Endpoint for Efficacy and Functioning Measures Figure 1. Patient Disposition CONCLUSIONS • Male and female outpatients at least 18 years of age • All patients must meet DSM-IV criteria for GAD with disease severity as follows: • Hospital Anxiety and Depression Scale (HADS) anxiety subscale score of ≥ 10 at Visit 1 • Clinical Global Impressions-Severity ≥ 4 at Visits 1 and 2 • Covi Anxiety Scale (CAS) score of ≥ 9; no item in the Raskin Depression Scale (RDS) > 3; and CAS score > RDS score • To be continued into double-blind phase, patients must meet response criteria: • Decrease ≥ 50% from baseline on the Hamilton Anxiety Rating Scale (HAMA) total score to ≤ 11 • Clinical Global Impressions of Improvement ratings of “much” or “very much improved” for the last 2 consecutive visits Purpose: To examine treatment with duloxetine 60–120 mg once daily for relapse prevention in adults with generalized anxiety disorder (GAD) using a 26-week open-label, flexible-dose acute therapy followed by a 26-week, double-blind, placebo-controlled, randomized withdrawal continuation phase. Methods: 887 patients ≥ 18 years of age [mean age = 43.3 yrs; 61% female] with a DSM-IV-TR‑defined GAD diagnosis entered open-label treatment with duloxetine 60–120 mg for 26 weeks. Treatment response was defined as a Hamilton Anxiety Rating Scale (HAMA) total score reduction from baseline ≥ 50% to a score of ≤ 11 and clinician improvement rating of “much” or “very much improved” for the last 2 visits of open-label treatment. Patients who completed open-label phase and met this definition were randomly assigned to receive either duloxetine (N = 216) or placebo (N = 213) for the 26-week double-blind continuation phase. Relapse was defined as an increase in the Clinical Global Impression Severity rating of at least 2 points from randomization (end of open-label phase) to a score ≥ 4 (moderate) while meeting criteria for GAD or by discontinuation due to lack of efficacy. Results: At the open-label endpoint, 78.8% of patients met the responder criteria and 44.3% met remission criteria (a HAMA total score ≤ 7). During the double-blind continuation phase, 41.8% of placebo-treated patients relapsed compared with 13.7% of duloxetine-treated patients (P ≤ .001). Among patients who did relapse, duloxetine-treated patients had a longer time to relapse compared with patients who were switched to placebo (log-rank test, P ≤ .001). On both primary and secondary measures, placebo-treated patients significantly worsened from randomization to study endpoint compared with duloxetine-treated patients in their illness severity and functioning (P ≤ .001, all comparisons). Discontinuation due to adverse events was 13.6% during open-label phase, and 1.9% in the double-blind continuation phase for duloxetine-treated patients. During the double-blind continuation phase, there was no significant difference between duloxetine and placebo groups in the frequency of emergent adverse events (P = .629), except for dizziness which was more frequent in the placebo group (9.9% vs 3.7%, P ≤ .05) for whom medication was withdrawn during the double-blind phase. Conclusions: The 3-fold greater relapse rate with placebo during the continuation phase indicates the need for on-going treatment for patients with GAD. Duloxetine was efficacious and well-tolerated for long-term treatment and significantly reduced the risk of relapse. • Among GAD patients who responded to duloxetine during 26-week open-label phase and then received double-blind treatment for 26 weeks, duloxetine 60–120 mg once daily was superior to placebo on the following endpoints: • Prevention of relapse (primary endpoint) • Change from baseline to endpoint on secondary efficacy and functioning measures • Duloxetine 60–120 mg once daily treatment was efficacious, associated with significantly lower relapse rates than placebo, greater maintenance of quality of life and daily functioning, and was generally well tolerated during this one year study. Key: HAMA, Hamilton Anxiety Rating Scale; HADS, Hospital Anxiety and Depression Scale; SDS, Sheehan Disability Scale; Q-LESQ-SF, Quality of Life Enjoyment and Satisfaction Scale Short Form a higher scores indicate greater worsening; b lower scores indicate greater worsening; *** P ≤ .001, between groups Key Exclusion Criteria • Diagnostic exclusions: • Any current and primary DSM-IV Axis I diagnosis other than GAD • Major depressive disorder within the past 6 months • Panic disorder, post-traumatic stress disorder, or an eating disorder diagnosis in past year • Lifetime diagnosis of obsessive-compulsive disorder, bipolar affective disorder, psychosis, factitious, or somatoform disorder • Medical exclusions: • Any medical condition that would contraindicate the use of duloxetine • Any excluded concomitant or psychotropic medication Figure 4. Adverse Events† Double-Blind Phase Adverse Events Open Label PhaseAdverse Events BACKGROUND • Generalized anxiety disorder (GAD) is a chronic disorder with low probability of spontaneous recovery1. • Long-term medication is often required for optimal management of GAD2. • Duloxetine has shown efficacy compared to placebo in 3 acute (9–10 week) therapy trials3,4,5. Outcome Measures RESULTS • Primary: Hamilton Anxiety Rating Scale (HAMA)6 • Secondary: • Hospital Anxiety and Depression Scale (HADS)7 • Clinical Global Impression Severity (CGI-S) and Improvement (CGI-I)8 • Functioning: • Sheehan Disability Scale (SDS) Global Functioning Score9 • Quality of Life Enjoyment and Satisfaction Scale (Q-LESQ-SF)10 Figure 2. Relapse Rate by Treatment (Double-blind Continuation Phase) * P ≤ .05 Study Objectives † Events occurring at frequency > 5% † Events occurring at frequency > 5% Primary: To examine the long-term efficacy of duloxetine 60–120 mg once daily for the prevention of relapse in patients with GAD who responded therapeutically to an initial 26-week course of duloxetine treatment. Secondary: To compare changes in efficacy and functioning measures between patients who were maintained on duloxetine with patients who were switched to placebo during the 26-week double-blind continuation phase. Serious Adverse Events Serious Adverse Events Statistical Analyses *** • Primary analysis compared time to relapse for duloxetine and placebo using a log-rank test. • Relapse was defined as ≥ 2-point increase in CGI-S ratings from double-blind randomization baseline to ≥ 4 (moderate) or as discontinuation due to loss of efficacy. • For most measures, differences between groups in the double-blind phase were examined using analysis of covariance (ANCOVA) model that included treatment and investigator as main effects and baseline score as a covariate. METHODS REFERENCES *** P ≤ .001 Study Design • Bruce SE. et al. Influence of psychiatric comorbidity on recovery and recurrence in generalized anxiety disorder, social phobia, and panic disorder: a 12-year prospective study. Am J Psychiatry 2005; 162:1179-1187 • Wittchen H.U., Hoyer J. Generalized anxiety disorder: Nature and course. J. Clin. Psychiatry 2001; 62,15–19, discussion 20–21. • Rynn M, et al. Efficacy and safety of duloxetine in the treatment of generalized anxiety disorder: a flexible-dose, progressive-titration, placebo-controlled trial. Depress Anxiety. 2007 Feb 20; [Epub ahead of print]. • Koponen H, et al. Efficacy of duloxetine for the treatment of generalized anxiety disorder: Implications for primary care physicians. Prim Care Companion J Clin Psychiatry. 2007;9:100-107. • Hartford J, et al. Duloxetine as an SNRI treatment for generalized anxiety disorder: results from a placebo and active-controlled trial. Int Clin Psychopharmacol. 2007;22:167-174. • Hamilton M. Development of a rating scale for primary depressive illness. Brt J Med Psych. 1959; 32:50-55. • Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scales. Acta Psychiatr Scand 1983; 67:361-370. • Guy W. The clinician and patient global severity and impression scales. In: ECDEU Assessment Manual for Psychopharmacology [76-338]. US Dept Health, Education, and Welfare, Rockville, MD;1976; pp. 218-222. • Sheehan D.V. The Anxiety Disease. Charles Scribner and Sons, New York;1983. • Endicott J., et al. (1993) Quality of Life Enjoyment and Satisfaction Questionnaire: a new measure. Psychopharmacol. Bull.29,321-326. Figure 3. Mean Hamilton Anxiety Rating Scale Total Score Table 1. Patient Demographics ACKNOWLEDGMENT We thank the patients who participated in the study. We would like to acknowledge our appreciation to the following principal investigators and their clinical research staff: Dr. Voker Arolt, Dr. Borwin Bandelow, Dr. Bertrand Baranosvsky, Dr. Benny Barnhard, Dr. Bettina Bergthold, Dr. J Alexander Bodkin, Dr. Joan Busner, Dr. Osvaldo Caro, Dr. WA de Backer, Dr. Anthony Dietrich, Dr. Bernadette D’Souza, Dr. Luisa Figueira, Dr. Christian Gaussares, Dr. Hermann-Josef Gertz, Dr. Francis Ghysen, Dr. Paul Gross, Dr. Thomas Gualtieri, Dr. Peter Halama, Dr. Ulrich Hegerl, Dr. Fritz Henn, Dr. Ethan Kass, Dr. Arif Khan, Dr. Saaid Khojasteh, Dr. Stephanie Kutler, Dr. Philippe Leclercq, Dr. Pierre Le Goubey, Dr. Robert Levine, Dr. Bruce Lydiard, Dr. Silva Marques, Dr. John Marshall, Dr. Carla Mendez, Dr. K Mulder, Dr. Pascal Pannetier, Dr. Franck Peyre, Dr. Jain Rakesh, Dr. Angelo Samubnaris, Dr. Thomas Shiovitz, Dr. Margot Schmitz, Dr. Martin Schuster, Dr. Georg Schonbeck, Dr. Andreas Strohle, Dr. Marques Teixeira, Dr. Mikel Thomas, Dr. Harry Van Mierilo, Dr. W Veerman, Dr. Hans-Peter Volz, Dr. Jim Whalen and Dr. Marcel Zins-Ritter. No significant differences between treatment groups in patients entering double-blind phase. a***P ≤ .001, within group; b***P ≤ .001, placebo vs. duloxetine. Poster presented at ACNP, Boca Raton, FL, USA; November 9-13, 2007