Download
1 / 5
50 likes | 185 Vues
Proper positioning during chest X-ray (CXR) is crucial for ensuring optimal results and patient safety. Key considerations include keeping the chin in a neutral position, aligning the body and shoulders, and ensuring the endotracheal tube (ETT) is out of the CXR field. Avoid flexing or extending the neck excessively, as this can distort ETT placement. Use the Z-flotation mattress judiciously and involve additional personnel for larger patients. Consultation with the provider prior to ETT re-taping and adherence to safety protocols during sedation are vital for effective airway management.

E N D
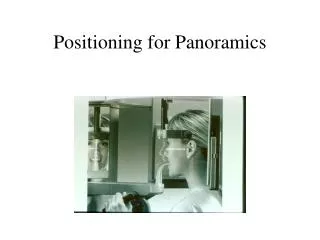
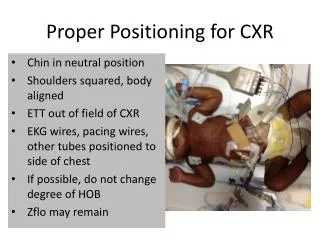
Proper Positioning for CXR Chin in neutral position Shoulders squared, body aligned ETT out of field of CXR EKG wires, pacing wires, other tubes positioned to side of chest If possible, do not change degree of HOB Zflo may remain
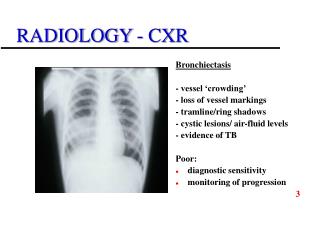
What’s wrong with this?? • ETT in CXR field (creates “shadow”) • Wires and tubes across chest • Neck is flexed • Neck in extended position causes the ETT to be too low on film • Neck in flexed position causes the ETT to appear high on film
Proper positioning creates the best possible film to reduce frequent ETT repositioning and multiple exposures as well as potential loss of airway. • Large Patient?? Get extra hands for lifting and holding airway. It is okay to shoot through the draw sheet. • It is not necessary to remove the Zflo on a smaller patient; flatten and put the Xray board on top • The providers would like the film shot in the HOB position in which the patient is usually positioned. • The bedside RN is responsible for ensuring the airway is stable throughout the Xray process. • Sedation might be required to keep your patient comfortable and in proper position. • You may need to wear the Xray shield and hold the patient in proper position.
PCCU Re-taping Checklist • There should be a conversation with Provider prior to re-taping any ETT • Does he/she wish to be present at the bedside • Does the patient have a “difficult airway”? (provider should be present) • What medications will be used to sedate and paralyze? Routine sedation/paralytic will be the standard for re-taping ETT in PCCU (if extubation is planned, extubate now instead of re-taping) • Are there copious secretions or other issues requiring assistance?
PCCU Re-taping Checklist (cont.) • Ensure that RT or provider increases RR on ventilator while paralytic in effect (and returns to decrease rate once pt. initiates spontaneous breaths) • Is there a bag/mask/suction at the bedside? • Suction mouth and hypopharynx prior to deflating cuff • Ensure cuff is deflated if ETT is to be repositioned • Use closed loop communication between RT and RN before final tape removed and throughout process: • “Are you ready to hold the ETT?” • “Yes, I have the ETT” • Holder should say STOP if he/she feels that the ETT is slipping