REFERENCES
Frequency of Swallowing Problems Experienced over the Last Month (Stage 1). ‘I am glad I had my feeding tube inserted’ (Stage 2). Sense of Wellbeing since Feeding Tube Inserted (Stage 2). Affects of Dysphagia and Gastrostomy Feeding on Quality of Life for People with Motor Neurone Disease


REFERENCES
E N D
Presentation Transcript
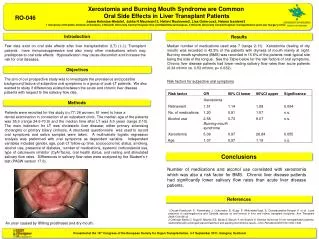
Frequency of Swallowing Problems Experienced over the Last Month (Stage 1) ‘I am glad I had my feeding tube inserted’ (Stage 2) Sense of Wellbeing since Feeding Tube Inserted (Stage 2) Affects of Dysphagia and Gastrostomy Feeding on Quality of Life for People with Motor Neurone Disease L. Doylea & K. McElligottb aDepartment of Speech & Language Therapy, bDepartment of Nutrition & Dietetics, Beaumont Hospital, Dublin, Ireland INTRODUCTION Motor Neurone Disease (MND), is a fatal, progressive, neurodegenerative disease of unknown aetiology, characterised by death of both upper and lower motor neurones1. Reduced oral intake frequently occurs in this patient group due to factors including dysphagia, poor appetite, extended meal times, reduced ability to self-feed, low mood and changes in taste. This often leads to ‘weight loss, malnutrition and dehydration which may aggravate muscle weakness, contribute to respiratory weakness, and perhaps shorten life span’2. The EFNS Task Force3 recommend that people with MND should be referred to a dietitian as soon as dysphagia appears. Intervention by a Speech and Language Therapist is also indicated to suggest alternative food/fluid consistencies and swallowing techniques. Initial nutritional interventions may include food fortification and nutritional supplementation. Gastrostomy insertion is also a routinely considered management option for this patient group. While the evidence for prolonged survival post-gastrostomy is weakly positive , a limited number of studies to date suggest that gastrostomy insertion has a possible positive effect on QOL4,5. OBJECTIVE To investigate to what extent dysphagia and gastrostomy feeding impacts on QOL for people with MND. METHOD Over an eighteen month period, people with MND who were scheduled for gastrostomy insertion in Beaumont Hospital completed a questionnaire at three stages. Prior to tube insertion (stage 1), participants (n=14) completed the SWAL-QOL, which is a validated questionnaire regarding the effects of dysphagia on QOL. This was repeated at approximately six weeks (stage 2) and six months (stage 3) following insertion. At stages 2 and 3, participants also completed the RIG-QOL (a questionnaire devised by the researchers to examine changes in wellbeing relating to gastrostomy feeding based on the format of the SWAL-QOL). • RESULTS • Participants reported an array of swallowing difficulties including choking on food and liquid as well as problems chewing. • At stage 1 (N=14), all participants felt dysphagia had a moderate or significant impact on their QOL. At stage 3 (N=4), all stated that dysphagia had a significant impact on their wellbeing and daily life. • All participants felt adequately involved in the decision to have a feeding tube inserted with 82% stating that this was ‘very much true’. • At stage 2 (N=11), all reported being at least ‘somewhat’ glad they had the feeding tube inserted while at stage 3 (N=4) all participants were ‘very’ glad that they had a gastrostomy. • At stage 2 (N=11), the main reported complications of gastrostomy tube feeding were reflux post-feeds and soreness around the stoma site, although only 1 participant reported that this was ‘almost always’ an issue. • All participants reported a better sense of wellbeing following gastrostomy insertion. ‘Considering all aspects of your health, overall how much of an impact does your swallowing difficulty have on your wellbeing and daily life?’ (Stage 1) DISCUSSION/CONCLUSIONS Dysphagia and malnutrition are factors which can negatively affect prognosis and QOL for people with MND. Changes in swallowing function and reduced oral intake can often be a significant source of fear and anxiety for both the person and their carers. In this study, all participants felt that their dysphagia had a negative impact on their QOL. While gastrostomy insertion may not significantly lengthen life expectancy for this patient group, it may have a positive impact on QOL. In addition to providing nutrition, gastrostomy tubes allow people with MND to continue taking medications and adequate fluids when it is no longer possible to do so orally. The current researchers acknowledge that due to the progressive nature of MND, it can be challenging to measure QOL concerning just one aspect of the condition. However, while the numbers in this study were small, this data indicates that people with MND who received gastrostomy feeding were glad they had a feeding tube inserted and felt some level of improved wellbeing. At stage 3 compared to stage 2, all remaining participants stated more strongly that they were glad they had a gastrostomy tube inserted. It may be that as the condition progresses, the benefits of a gastrostomy tube become more apparent to people with MND. More research is needed in this area to further examine the affects of gastrostomy feeding on QOL for people with MND across a larger group of participants. REFERENCES 1. Karitzky J, Ludolph AC. Imaging and neurochemical markers for diagnosis and disease progression in ALS. Journal of the Neurological Sciences 2001;191(1-2):35–41. 2. Katzberg HD & Benatar M. Enteral tube feeding for amyotrophic lateral sclerosis. Cochrane Database Systematic Review, 2011;(1):CD004030. 3. Anderson PM Abrahams S, Borasio GD, De Carvalho M, Chio A, Van Damme P, Hardiman O, Kollewe K, Morrison KE, Petri S, Pradat PF, Silani V, Tomik B, Wasner M & Weber M. EFNS guidelines on the clinical management of Amyotrophic Lateral Sclerosis (MALS) – revised report of an ENFS task force. European Journal of Neurology. 2012;19(3);360-375. 4. Mazzini L, Corra T, Zaccala M, Mora G, Del Piano M, Galante M. Percutaneous endoscopic gastrostomy and enteral nutrition in amyotrophic later sclerosis. J Neurol 1995;242:695-8. 5. Mitsumoto H, Davidson M, Moore D, Gad N, Brandis M, Ringel S et al. Percutaneous endoscopic gastrostomy (PEG) in patients with ALS and bulbar dysfunction. Amyotrophic Lateral Sclerosis and Other Motor Neurone Disorders 2003;4(3):177-85.