Visual Evoked Potentials
Visual Evoked Potentials. Electrophysiological Assessment of Visual Cortical Functioning. E. Eugenie Hartmann, PhD School of Optometry. Advantages of Electrophysiology. Objective (??) Non-Invasive. Finding the Signal. EEG = On-going electrical activity Visual Signal = Elicited Response.

Visual Evoked Potentials
E N D
Presentation Transcript
Electrophysiological Assessment of Visual Cortical Functioning E. Eugenie Hartmann, PhD School of Optometry
Advantages of Electrophysiology • Objective (??) • Non-Invasive
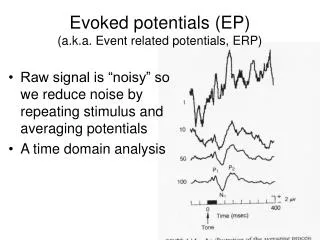
Finding the Signal • EEG = On-going electrical activity • Visual Signal = Elicited Response
Principles of Electrophysiology • detection of electrical activity • signal averaging • voltage versus time • two-dimensional waveforms
Generation of responses • neural activity • localized regions become depolarized or hyperpolarized • creates “sinks” or sources of current
Visual Electrodiagnostics • Retinal Functioning • ERG Electroretinogram • EOG Electro-oculogram • Optic Nerve and Cortical Functioning • VEP Visual Evoked Potential
Confirmation of (Early) Disease • testing may be helpful • to confirm the diagnosis • to rule out alternative diagnoses
VEP VEP Visual Evoked Potential VER Visual Evoked Response VECP Visual Evoked Cortical Potential
VEP • Assesses visual pathway • From optic nerve to V1 • Spatial visual processing in pre-verbal and non-verbal individuals
V1 Topography Contributes to Foveal Dominance cortical magnification of the representation of the fovea approximate cancellation of dipoles in periphery Butler, 1987
Photic Driving is a Crude VEP Chiappa, 1979
Signal to Noise is Proportional to the Square Root of the Number of Averages Number of averages Chiappa
Latency and Amplitude Measurements Spehlmann, 1985
VEP Waves and Generators • N70: standing wave, thalamocortical input • P100: standing wave, intracortical inhibition in striate cortex but also extrastriate activity. This is the most robust component. • N145 and later components: standing wave, striate and extrastriate activity These waves are foveally-dominated, especially for small checks or fine gratings. Striate cortex dominates N70 and P100, but extrastriate cortices are active.
VEP Criteria for Abnormality • P-100 latency prolongation • Absent VEP • P-100 interocular latency difference • P-100 interocular amplitude difference, only if at least 4:1 • Abnormal waveform (if monocular)
Types of VEP RecordingsSpatial Domain Flash Pattern spatial variations contrast variations
Swept-parameter VEP • Pattern changes rapidly contrast spatial dimension • Grating steady-state • Checkerboard transient
Steady-state Sweep VEP • Gratings • 1-second per pattern size • 6 different gratings • 5 - 10 sweeps averaged
7/28/1999 5 RUNS (FIRST 5) OD SFSQ5E SUBJECT: JF991 AGE: 24 weeks VD =114 cm SF C/D 2-3 = * 3-4 = * 4-5 = 11.03 5-6 = * Steady-state Sweep VEP • Grating Sweep, 7.5 Hz • 5 runs • JF991 24 weeks OD JF991 24 weeks OS • Acuity = 11.03 cpd Acuity = 10.62 cpd Spatial Frequency (cpd)
Effect of Fatty Acids on Acuity Measured with VEP Human breast milk AA and DHA added Standard Formula
Check Size Determines Effective Spatial Contrast 1/8 deg (7.5 min) 1/4 deg (15 min) 1 deg (60 min) 4 deg (240 min) 8 deg (480 min) 2 V 25 msec very small checks: below resolution of many receptive fields Cz-Oz very large checks: few contours, C and S act antagonistically
VEP Criteria for Abnormality • P-100 latency prolongation • Absent VEP • P-100 interocular latency difference • P-100 interocular amplitude difference, only if at least 4:1 • Abnormal waveform (if monocular)
Factors that alter P100 waveform in normal subjects: Visual acuity (<20/200 for P100 to be abnormal) Pupillary size (causes interocular latency difference) Age (latency increase with age especially after 60) Sex (females have typically shorter latencies than males) Subject cooperation
Normal VEP 32 y.o., r/o MS 20/20 OS20/20 OD 1/2 deg (30 min) stim OS stim OS Cz-Oz Cz-Oz P100 latencies are similar in the two eyes stim OD stim OD 1/4 deg (15 min) P100 latency increases slightly with smaller checks 5 V 25 msec
Effect of Defocus No lens: 20/15 +1D: 20/20 +2D: 20/40 +2.5D: 20/100 Substantial defocus will prolong latency and reduce amplitude due to reduction in retinal contrast. 3 V 25 msec 1/4 deg (15 min) Cz-Oz
Unilateral Delay 20 y.o., r/o MS 20/20 OS20/20 OD stim OS 1/2 deg (30 min) Cz-Oz 15 V stim OD 25 msec P100 prolonged, but amplitude preserved Substantial interocular latency difference
Small Check Size Increases Sensitivity 25 y.o., r/o MS 2 deg (120 min) 20/40 OS20/20 OD 1/2 deg (30 min) stim OS Cz-Oz 1/4 deg (15 min) Normal P100 and no interocular difference stim OD 5 V 25 msec Significant interocular latency difference
Acute Demyelination and Recovery acute attack OS 30 y.o., MS 20/400 OS20/20 OD stim OS stim OS 1/2 deg (30 min) 5 mos later 6 yrs later Cz-Oz Cz-Oz 20/40 OS20/20 OD 20/20 OS20/20 OD stim OD stim OD demyelination and recovery OS asymptomatic attack OD 4 deg (240 min) 5 V 25 msec