Download

1 / 21
210 likes | 710 Vues
Monitoring of motor evoked potentials in C-spinal surgery. 報告人: R1 康庭瑞. Case. Chart No: 4213769 Brief history:

E N D
Monitoring of motor evoked potentials in C-spinal surgery 報告人:R1康庭瑞
Case • Chart No: 4213769 • Brief history: 1. The 19 y/o man had suffered from TA in May,2002 and multiple trauma, including right F-T-P EDH with depressed skull fracture, left F-T-P SDH and ICH, and type II odontoid fracture was noted. 2. Emergency craniotomy and hematoma evacuation were done at that time.
Case 3. Cranioplasty in June,2002; odontoid screw fixation in July; screw removal due to mal-alignment of odontoid process on August 6th; posterior bone fusion and Halifax fixation of C1-2 on August 12th; and right Kocher VP shunt on August 23th,2002 at 光田 hospital 4. After operation, GCS:E4M6V2 5. He received cranioplasty with mini-plate fixation on November at NTUH 6. This time, he was admitted for removal of C1-2 Halifax, C1 laminectomy and lugue fixation C0-3 with bone fusion
Spinal surgery • Induction: Fentanyl 100ug, Pentothol 300mg, Atracurium 40mg • Intubation: lightwand stylet • Monitors: pulse oximetry, ECG, capnography, invasive blood pressure, CVP, MEP • Position: prone positionendotracheal tube position and fixation, free of pressure • Maintain: total intravenous anesthesiaPropofol, Ketamine+Rapifan, Esmeron
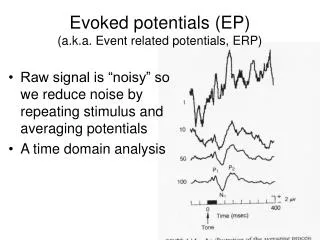
Somatodensory evoked potentials • Standard test of spinal cord function during various surgical proceduresdorsal and lateral columns; good correlation between SSEP and motor function • The upper extremity SSEP monitor the brachial plexus, essential during procedures of the cervical spine, indirectly monitor peripheral nerve function • The lower extremity SSEP assess overall spinal cord function • Criteria for significant changes in waveform:10% latency increase, 50% decrease in signal amplitude, and/or complete loss of potential
Motor evoked potentials (1) • Stimulation techniques: (1) transcranial magnetic or electrical stimulation of the cerebral cortex (2) direct(epidural) or indirect(percutaneous) stimulation of the spinal cord • Recorded: (1) from spinal cord using epidural electrodes (2) from mixedperipheral nerves using surface or subdermal electrodes neurogenic action potentials (3) from muscle compound muscle action potentials
Motor evoked potentials (2) • Vascular injury to the anterior spinal cord can occur motor deficit without a change in the sensory potential • Intramedullary spinal cord tumor resection, vascular abnormalities, and correction of spinal deformity • Absence of the MEPs remedy and if no recovery of EPs wake-up test
Drawbacks of transcranial MEP • Technically more demanding than SSEP • Transcranial stimulation remains a controversial topic • Lack of significant criteria for warning except neurogenic action potentials
Confounding factors • Anesthetics: volatile anesthetics reducing amplitude, prolonging latency of EPs • Temperature: hypothermia • Hypotension • Hypoxia cerebral ischemia • Anemia • Preexisting neurologic lesions
Inhalation agents • Greatest depressive effect on evoked potentials • Dose-dependent prolong the latency and decrease the amplitude of EP • N2O decrease the amplitude of EP but have minimal effect on the latency of EP
Intravenous anesthetics • Less effects on evoked potentials • Thiopental, opioid and propofol depress MEP to a greater extent than do etomidate or methohexital • A 2-mg/kg dose of thiopental decreased the MEP amplitude 42.8 percent, and subsequent doses caused a further dose-dependent decrease • Ketamine does not follow the basic anesthesia-related EEG pattern, and was desirable for MEP monitoring
Our anesthetic formula for MEP monitoring • Ketamine 200mg + Rapifen 2mg in 20ml N/S run 10~12 ml/hr • Propofol 70mg//hr • Esmeron 6mg/hr
Conclusion • Selection of adequate neuromonitoring during spinal surgery is important • Totally intravenous anesthesia and short acting agents is better • Maintain anesthesia depth: TOF for controlling muscle relaxant dosage; BIS or EEG for monitoring hypnosis
Reference • Combined monitoring of motor and somatosensory evokedpotentials in orthopaedic spinal surgery. [Clinical Trial. Journal Article] Clinical Neurophysiology. 2002 Jul. • Transcranial electrical motorevoked potential monitoring for brain tumor resection. [Journal Article] Neurosurgery. 2001 May. • Spinal cord and nerve root monitoring during surgical treatment of lumbar stenosis. [Review]Clinical Orthopaedics & Related Research. 2001 Mar. • Total intravenous anesthesia for intraoperative monitoring of motor pathways : an integral view combining clinical and experimental dataJournal of Neurosurgery 2002 Mar • Effects of four intravenous anesthetic agents on motor evoked potentials elicited by magnetic transcranial stimulation. Neurosurgery 1993