Download
1 / 152
1.56k likes | 2.02k Vues
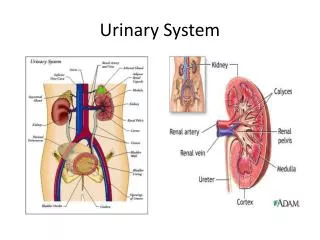
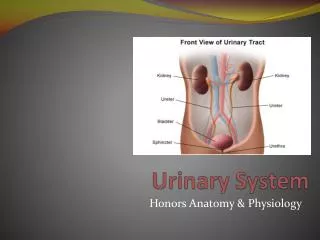
DR.Sh.Sajjadieh nephrologist. SIGNS & SYMPTOMS OF URINARY SYSTEM. PROTEINURIA. Protein. Abnormal quantity of protein excretion in the urine is called proteinuria . 95% of normal adults excrete less than 150 mg/d. Children and adolescent can excrete up to 250 mg/d.

E N D
DR.Sh.Sajjadieh nephrologist SIGNS & SYMPTOMS OF URINARY SYSTEM
Protein • Abnormal quantity of protein excretion in the urine is called proteinuria. • 95% of normal adults excrete less than 150 mg/d. • Children and adolescent can excrete up to 250 mg/d. • Higher rates of protein excretion that persist beyond a single measurement should be evaluated.
Proteinuria • Proteinuria is defined as urinary protein excretion exceeding 2 SD from the mean. Normal values depend upon the age • Premature neonates 140 mg/m2/d full term neonates 70 mg/m2/d Children <10 yr 150 mg/d Children 10-18 yr 300 mg/d Adults 150 mg/d
Normal Proteinuria • 30 to 150 mg/day • Usually only small proteins (<20,000 daltons) pass across capillary wall and most are reabsorbed in prox. tubules e.g., a2-microglobulin, apoproteins, enzymes, peptide hormones • Tamm-Horsfall protein (uromodulin) • High m. wt. 23 x 106 daltons glycoprotein • Thick ascending limb and distal convoluted tubule • IgA and urokinase in small amounts
Sources of abnormal proteinuria: • Disruption of glomerular capillary barriers (high m. wt. proteinuria) • Tubular damage, inability of prox. tubule to reabsorb normally filtered proteins (low m. wt. proteinuria) • Increased production of normal and abnormal plasma proteins which are filtered and inadequately reabsorbed • Increased tubular production of protein
Reagent Strip Tests for Protein • PH indicators change color with protein • Sensitive for albumin but not immunoglobulins • Strongly pigmented urine interferes with color reaction (hyperbilirubinemia, pyridium) • False positives in very alkaline urine • Sensitivity, 32-46% using 25 mg/dLproteinuria
Sulfosalicylic Acid (SSA) Method • Cold precipitation of proteins with a strong acid - urine will become turbid, measured by photometry • Poor precision - coefficient of variation is 20% • Gamma globulins and albumin detected, more sensitive to the latter • Substituting trichloracetic acid results in more sensitivity for gamma globulins
False Positive Sulfosalicylic Acid (SSA) Test • Turbidity of urine from another cause • Radiographic contrast dye (high SG on urinometer but normal dipstick) • Penicillin, cephalosporin, sulfonamides, tolbutamide, tolectin • False negative in alkaline urine
Discordance between SSA and Reagent Strip • If SSA is positive while dipstick reagent is negative - non albumin proteinuria is suspected (e.g., gamma globulin paraproteins) -Pancreatic transplant patients, nonalbumin pancreatic enzymes in urine
Sensitive Methods for Urine Albumin • Radioimmunoassay – double antibody technique • Immunoturbidometric technique - albumin + antibody create a turbid mixture measured by spectrophotometry • Albumin - antibody complexes measured by laser nephelometer • ELISA
Urinanalysis • 70-80% of excreted protein is in upright position. • The urine dipstick for protein primarily detects albumin.
Urinanalysis • In normal urine, 60% of the proteins originate from the plasma and other 40% from the kidney and urogenitaltract. • Normal protein composition is approximately 40%albumin, 40% Tomm-Horsfal protein, 15% immunoglobulins, 5% other plasma proteins.
Urinanalysis • Dipstick is simplest and least expensive method. • It detects protein concentration > 20 mg% and depends on urine concentration and is insensitive to globulin. • False positive in highly alkaline urine, presence of bacteria, blood, ammonium compounds, or chlorhexidine.
Urinanalysis • Sulfosalicylic acid is more sensitive (down to 5 mg%) and react equally with albumin and globulin.
Urinanalysis • False positive results can occur if the urine contains tolbutamide, radiocontrast agents, or high level of cephalosporin, penicillin, or sulfonamides.
Urinanalysis • Quantitatively method is urine electrophoresis. • At times, it is necessary to quantify protein excretion; determining the 24-hour protein collection, or protein to creatinine ratio.
Urinanalysis • Microalbuminuria refers to elevated urine albumin excretion that is below the level of detection (30-300 mg/d or 20-200 mg/min) by routine urine protein dipstick test.
TYPES OF PROTEINURIA • There are three basic types of proteinuria : glomerular, tubular, and overflow. • Only glomerularproteinuria (ie, albuminuria) is identified on a urine dipstick.
Glomerularproteinuria : • the proteinuria in glomerular disease is due to increased filtration of macromolecules (such as albumin) across the glomerular capillary wall.
Tubular Proteinuria • Low molecular weight proteins ( such as microglobulin, immunoglobulin light chains, retinol-binding protein, and amino acids) have a molecular weight that is generally under 25,000 in comparison to the 69,000 molecular weight of albumin.
Tubular Proteinuria • These smaller proteins can be filtered across the glomerular and are then almost completely reabsorbed in the proximal tubule.
Tubular Proteinuria • Interference with proximal tubular reabsorption, due to a variety of tubulointerstitial diseases or even some primary glomerular diseases, can lead to increased excretion of these smaller proteins.
Tubular Proteinuria • Tubular proteinuria is not diagnosed clinically since the dipstick for protein does not detect low molecular weight proteins and the quantity excreted is relatively small.
Overflow Proteinuria • Increased excretion of low molecular weight proteins can occur with marked overproduction of a particular protein (almost always immunoglobulin light chains in multiple myeloma) • In this setting, the filtered load is increased to a level that exceeds the normal proximal reabsorptive capacity.
Tissue Proteinuria • Abnormal protein excretion due to tissue or tumor necrosis.
Isolated proteinuria • Proteinuria without hematuria or an elevated serum creatinine concentration • asymptomatic and the presence of proteinuria is discovered incidentally. • This is different from that in patients with more prominent renal disease who have one or more of the following: heavy proteinuria(>3 g/day), lipiduria, edema, and/or an active urine sediment containing red cells (which are often dysmorphic) and red cell casts.
Annual screening for proteinuria is not cost-effective in the general population of healthy individuals under age 60. • Routine urinalysis is recommended for high risk patients :diabetes or hypertension • Early detection of proteinuria in high risk patients is important because the administration of an ACE inhibitor or ARB → slow the progression of proteinuric chronic kidney disease.
Glomerularproteinuria • Almost all cases of persistentproteinuria are due to glomerularproteinuria. • Increased filtration of macromolecules (such as albumin) across the glomerular capillary wall : diabetic nephropathy and other glomerular diseases orthostatic or exercise-induced proteinuria • Most patients with benign causes of isolated proteinuria excrete less than 1 to 2 g/day
Tubular proteinuria • Low molecular weight proteins :ß2-microglobulin, immunoglobulin light chains,, and amino acids — have a molecular weight that is generally under 25,000 can be filtered across the glomerulus and are then almost completely reabsorbed in the proximal tubule. • The increased excretion of immunoglobulin light chains (or Bence Jones proteins) in tubular proteinuria is mild, polyclonal (both kappa and lambda), and not injurious to the kidney. This is in contrast to the monoclonal and potentially nephrotoxic nature of the light chains in the overflow proteinuria seen in multiple myeloma.
Overflow proteinuria • Increased excretion of low molecular weight proteins can occur with marked overproduction of a particular protein, leading to increased glomerular filtration and excretion. This is almost always due to immunoglobulin light chains in multiple myeloma, but may also be due to lysozyme (AML), myoglobin (in rhabdomyolysis), or hemoglobin (in intravascular hemolysis) .
Some patients have mixed forms of proteinuria: • Patients with myeloma kidney also may develop a component of tubular proteinuria, since the excreted light chains may be toxic to the tubules, leading to diminished reabsorption. • Glomerular diseases such as focal segmental glomerulosclerosis can be associated with proximal tubular injury, leading to tubular proteinuria.
MEASUREMENT OF URINARY PROTEIN • Standard urine dipstick • Detection of albumin via a colorimetric reaction between albumin and tetrabromophenol blue producing different shades of green according to the concentration of albumin in the sample. • The dipstick is insensitive to the presence of non-albumin proteins. • positive dipstick usually reflects glomerularproteinuria. • Pure tubular or overflow proteinuria will not be diagnosed unless a 24-hour urine is collected for some other reason, or the urine is tested with sulfosalicylic acid which detects all proteins.
…MEASUREMENT OF URINARY PROTEIN • Both the dipstick and sulfosalicylic acid test will detect urinary lysozyme (AML). Thus, lysozyme excretion should be measured in this setting, particularly if other signs of the nephrotic syndrome (such as edema and hyperlipidemia) are absent. • The results with the dipstick and SSA serve as only a rough guide of the degree of protein excretion since urine concentration will affect the measurement.
Measurement of quantitative protein excretion • Determination of the degree of protein excretion is a central part of the evaluation of patients with acute and chronic kidney diseases • The degree of proteinuria is prognostically important in patients with a primary glomerular disease. Most patients with the benign forms of isolated proteinuria excrete less than 1 to 2 g/day. • The degree of proteinuria is used to monitor the response to therapy.
…Measurement of quantitative protein excretion • Most patients with persistent proteinuria should undergo a quantitative measurement of protein excretion. • 24-hour urine measurement; however, collecting these specimens is cumbersome in ambulatory care settings. • Random urine specimen to estimate the degree of proteinuria .This test calculates the total protein-to-creatinine ratio (mg/g). This ratio correlates with daily protein excretion expressed in terms of g per 1.73m2 of body surface area .
…Measurement of quantitative protein excretion • It is important to note the units of measurement in your laboratory. If the urinary creatinine concentration is measured in mmol/L, the formula must be amended as follows, since 1 mg/dL equals 0.088 mmol/L: • Protein excretion = (Urine [protein] x 0.088) ÷ Urine [creatinine]
Microalbuminuria • Microalbuminuriais defined as persistent albumin excretion between 30 and 300 mg/day (20 to 200 µg/min). • The normal rate of albumin excretion is less than 20 mg/day (15 µg/min). • The standard urine dipstick is an insensitive method to detect microalbuminuria, which is the earliest clinical manifestation of diabetic nephropathy and, in patients without diabetes, is a marker of increased cardiovascular risk. • Dipsticks are available that detect the urine albumin concentration in this range, but the preferred test for diagnosis and monitoring is the urine albumin-to-creatinineratio.
Examination of the urine • The urine sediment should be examined for other signs of glomerular disease such as hematuria, red cell casts, or lipiduria and Red cell casts. • If the sediment is unremarkable, the differential diagnosis includes transient proteinuria, orthostatic proteinuria, and persistent proteinuria. • The urine dipstick should be repeated on at least one other visit. If these subsequent tests are negative for protein, the likely diagnosis is transient proteinuria.
Rule out transient proteinuria • Transient proteinuria is common: (fever and exercise) With marked exercise, the excretion of both albumin and low molecular weight proteins is increased, suggesting both an increase in glomerular permeability (to allow the filtration of albumin) and a reduction in proximal reabsorption.
Rule out orthostatic proteinuria • If the patient is younger than age 30 and has documented proteinuria on more than one occasion. This test detects orthostatic proteinuria, a relatively common finding in adolescents (occurring in 2 to 5 percent), but an uncommon disorder in those over the age of 30 . • Orthostatic proteinuria is characterized by increased protein excretion in the upright position, but normal protein excretion when the patient is supine ?neurohumoral activation and altered glomerular hemodynamics • Total protein excretion is generally less than 1 g/day in orthostatic proteinuria, but may exceed 3 g/day in selected patients.
…Rule out orthostatic proteinuria • Orthostatic proteinuria is a benign condition requiring no further evaluation or specific therapy .In many patients, the condition resolves over time. • Many patients with glomerular disease will have a modest reduction in protein excretion when supine. However, the diagnosis of orthostatic proteinuria requires that protein excretion be normal when supine (less than 50 mg per 8 hours), not merely less than when in the upright position
…Rule out orthostatic proteinuria • Split urines are collected according to the following protocol . • A 16-hour upright collection is obtained between 7 AM and 11 PM, with the patient performing normal activities and finishing the collection by voiding just before 11 PM. (The times can be adjusted according to the normal times at which the patient awakens and goes to sleep.) • The patient should assume the recumbent position 2 hours before the daytime collection is finished to avoid contamination of the supine collection with urine formed when in the upright position. • A separate overnight 8 hour collection is obtained between 11 PM and 7 AM.