Download
1 / 13
130 likes | 574 Vues
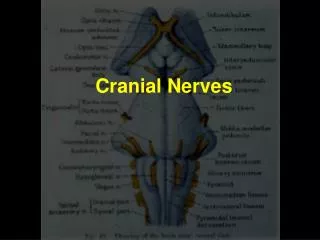
Examination of the Cranial Nerves. Dr Sarah Jones Manchester Royal Infirmary Clinical Skills Department. Objectives. To be able to perform a fluent examination of the cranial nerves and summarise findings Again, not about pathology. I: OLFACTORY. Rarely tested as limited clinical value

E N D
Examination of the Cranial Nerves Dr Sarah Jones Manchester Royal Infirmary Clinical Skills Department
Objectives • To be able to perform a fluent examination of the cranial nerves and summarise findings • Again, not about pathology
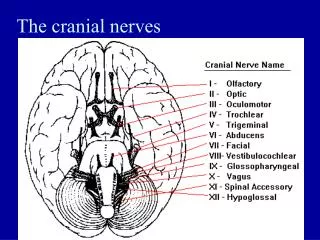
I: OLFACTORY • Rarely tested as limited clinical value • Bottles tend to exist in academic situations
II: OPTIC • Visual acuity (corrected, brain not lens) • Colour vision • Visual fields and blind spot • Retinal part of fundoscopy • Pupillary response – 2nd nerve afferent, 3rd nerve efferent
III, IV, VI: OCULOMOTOR, TROCHLEAR, ABDUCENS • Inspection of eyelids and pupils for ptosis, asymmetry, etc • Pupillary response – direct and consensual • Near reaction • Conjugate eye movements, saccades, nystagmus • (IV – superior oblique, VI – lateral rectus)
V: TRIGEMINAL • Sensory and motor • 3 divisions • Sensory in opthalmic, maxillary, mandibular • Corneal response • Jaw jerk • Masseter and temporalis – palpate and test power
VII: FACIAL • Sensory to anterior 2/3 tongue and external ear • Motor to the muscles of the face and lacrimal ducts • Ask about taste and eye watering • Ask patient to screw eyes up tight and open wide
VIII: AUDITORY • Ask patient to occlude opposite ear • Auditory function – should be able to hear whispering/ watch/ fingers at 0.75m • Rinne’s test (what’s a positive?) • Weber’s test • Test for positional vertigo/ nystagmus (often omitted)
IX: GLOSSOPHARYNGEAL • Clinically – only the gag reflex is testable • Usually omitted as unpleasant and isolated lesions very rare
X: VAGUS • Most branches to the throat and abdominothoracic viscera • Clinically- assess movements of the uvula and posterior pharyngeal wall • Deviation is away from the lesion
XI: ACCESSORY • Has cranial and spinal components • Only spinal can be assessed • Test power in sternomastoid and trapezius
XII: HYPOGLOSSAL • Motor to the tongue • Inspect • Ask patient to protrude tongue • Assess lateral movements • Assess power