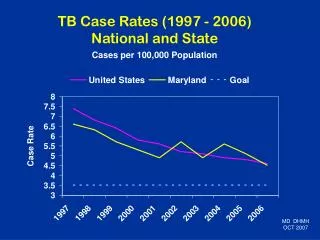
ALL CASE RATES
ALL CASE RATES. Governing Policies in the Shift of Provider Payment Mechanism From Fee-For-Service to Case-Based Payment. All Case Rates Policy NO. 1. BASES IN THE R.A. 7875. “Universality”. “Equity “. “Effectiveness”. “Cost Sharing “. “Cost Containment”. WHY REPLACE FEE FOR SERVICE.


ALL CASE RATES
E N D
Presentation Transcript
Governing Policies in the Shift of Provider Payment Mechanism From Fee-For-Service to Case-Based Payment All Case Rates Policy NO. 1
BASES IN THE R.A. 7875 “Universality” “Equity “ “Effectiveness” “Cost Sharing “ “Cost Containment”
WHY REPLACE FEE FOR SERVICE • Inefficient • Overutilization of diagnostic procedures • Unnecessary health care services • Wasteful payments • Inequity when comparing payments to private and government health care institutions And because...
COUNTRIES WORLDWIDE HAVE BEGUN TO SHIFT TO CASE-BASED PAYMENT SOURCE: “Case-Based Hospital Payment Systems: A Step by Step Guide for Design and Implementation in Low and Middle Income Countries” – Cashin, et. al, USAID from the American People, December 2005
General Objectives • To phase out fee-for-service payment mechanism • To simplify reimbursement rates understood by all sectors • To improve turnaround time of processing of claims
Scope and Coverage • Case rate payments shall be uniformly applied to all medical conditions and procedures, regardless of member category, that are admitted in accredited health care institutions. • It shall also apply to all identified day surgeries and select procedures done in accredited health care institutions. • It shall also be applied to directly filed claims by members subject to compliance to rules on direct filing.
WHAT WILL THE CIRCULAR CHANGE? The Fee-for-Service (FFS) system shall be replaced by CASE-BASED payment.
WHAT WILL BE THE EFFECTS? • PhilHealth members shall have a much reduced out-of-pocket spending as compared to non-PhilHealth members IF Case Rate (CR) reimbursements is NOT construed as an add-on • All CR payments shall be paid to the account of the HCI. • HCI to pay health care professionals (HCP) not exceeding 30 calendar days • Credentialing and Privileging of doctors shall be delegated to the HCI • HCI shall withhold the expanded withholding tax, VAT, as per BIR policy
WHAT WILL BE THE EFFECTS? • PhilHealth shall NO longer have tiered payments according to training or specialization of the doctors. • Direct filing by members shall only be allowed under certain circumstances. • NBB policy shall apply to ALL CASES, no longer confined to the initial 23. • Post Audit Monitoring is Institutionalized- replacing Pre-Audited Claims Processing
HOW WERE THE RATES DETERMINED?
Methodology • COSTING • using 2 sets of codes: • ICD 10 for medical conditions • RVS for procedures • GROUPING • condition of similar nature and management • were grouped together
Methodology Condition Case Rates • Why AVPC? • Source of available data is PHIC dbase • No fair costing studies on PF and hospital charges
Facility Fee: Average hospital fee per RVU +20% Professional Fee: RVU-based rates = RVU x 56 x1.5 Methodology Procedure Case Rates • Why RVU? • To make PF rate Commensurate to the level expertise of doctors and receive what they used to get from PHIC
Methodology • Conditions of similar nature and management were grouped together • Review of grouping and rates • Objective: to validate the ICD codes within the group and rates of the group; to determine if effect of proposed policies to the grouping and vice versa; • Specialty societies were asked to submit a list of their most commonly claimed conditions and procedures • Comparison of IPT proposed rates with rates from specialty societies • Consultation with societies to verify/validate groups and identify admissions criteria • Adjust groups and rates based on consultation • Actuarial evaluation and projection on proposed case rates
Support to Universal Health Care We, the (Name of Society), support the Philippine government thru the Department of Health (DOH) and the Philippine Health Insurance Corporation (PhilHealth) in the pursuit of Universal Health Care (UHC) known as KalusuganPangkalahatan (KP). We understand that the achievement of KP is premised on an improved way of provider engagement through a more transparent and efficient provider payment mechanism that is the case rates payment scheme. We understand that case rates promote equity and financial risk protection especially through the implementation of the No Balance Billing (NBB) Policy for the poor under the Sponsored Program. In support of KP, we, the (Name of Society) support the implementation of case rates.
Consultations with Specialty Societies, Professional Groups, Hospitals, Non-Government Organizations and Other Experts
Includes PMA, PCP, PCS, PPS, PAFP, POGS, PCR, DOH-retained hospitals
Presentation of the All Case Rates Message, Sample Groups and Rates Discussion of issues on payment of professional fees, credentialing and privileging and quality care
23 medical specialty societies signed the Support to Universal Health Care (UHC) document including the major societies – PMA, PCP, PCS, PPS, PAFP, PSA
General Policies • The FFS is being phased out and the preferred mode shall be case rates. All claims for medical conditions and procedures submitted to PhilHealth shall be paid using case rates. • All ICD and RVS codes will be given rates • The objective is to reduce the out-of-pocket expenditures of patient-members. In no instance, therefore, shall case rates be added to the expenses. • CR payment not an add-on to hospitalization and PF fees
General Policies • For certain surgical procedures, in order to promote better efficiency and the most modern interventions, patient admission may not be necessary in the provision of complete quality care. Thus, these surgical case rates shall be paid in full whether done as inpatient or outpatient (i.e., day surgeries). A list of these procedures shall be specified in the implementing guidelines.
General Policies • All Case Rate Reimbursement will be paid to HCIs. • HCI shall be accountable to PHIC for all that happens to the patient while under their care • HCI to facilitate the payment to health care professionals (HCP) not exceeding 30 calendar days upon receipt of the reimbursement or to a time frame as agreed upon by the specific facility management and their professionals. • PhilHealth shall regularly inform the HCPs of payments made to the HCI through a furnished copy of the Notice of Paid Claims and/ or Notice of Denied Claims (through email) • HCI as the withholding tax agent for PF fees • withhold the expanded withholding tax and the final value added tax (VAT) on Government Money Payment (GMP), if applicable • PhilHealth shall withhold the income tax as per BIR policy against the case rate amount to be paid to the HCI
General Policies • Credentialing and privileging of doctors (including specialists), and other health care professionals shall be delegated to the concerned HCI. Hospitals will deduct PHIC benefit for eligible patients and file the claims within 60 days except for direct claims • No more tiered payments according to training or specialization of the doctors • HCIs shall be responsible to file the claims of PhilHealth beneficiaries within the prescribed period of filing (60 days). • Direct filing by members shall only be allowed for certain circumstances as prescribed by PhilHealth.
General Policies • The No Balance Billing (NBB) policy shall apply to all indigents and sponsored sectors. • The Corporation shall set specific case rate guidelines for the following special circumstances: • Geographically Isolated and Disadvantaged Areas (GIDA) • Health Human Resource Shortage areas • Emergency/ acute care - selected emergency department visits that are skilfully evaluated and efficiently managed without need for further admission • Other special circumstances as determined by the Corporation
Implementing Guidelines on Medical and Procedure Case Rates ACR Policy No. 2
IV. General Rules • The case rates shall be the only reimbursement rates for all specified cases. These rates shall be the amount to be paid to the health care institutions and shall include the professional fees (PF). Medical conditions and procedures that are not in the list shall no longer be reimbursed • Admission due to patient’s choice shall NOT be reimbursed by the Corporation
IV. General Rules • Case rate payments shall cover for • Professional fees • HCI charges, including but not limited to: • room and board • diagnostics and laboratories • drugs/medicines • supplies • operating room fees • other fees and charges • Pre-operative diagnostics done prior to confinement are not covered.
IV. General Rules • Computation of Reimbursement • Professional Fees • Health Care Institutions • Single Period of Confinement • Forty-Five Days Benefit Limit • Special Reimbursement Rules • Additional Conditions for Entitlement • Computation of Taxes • Quality Standards
IV. D. Computation of Reimbursement • For MEDICAL case rates, the HCI fee and the PF shall be 70% and 30% of the case rate amount respectively
IV. D. Computation of Reimbursement • For procedure case rates, the following shall be the basis for computation except for specified cases: • PF = RVU x 56 x 1.5 (except for specified procedure case rates) • HCI fee = case rate amount - PF
IV. D. Computation of Reimbursement • A list of the complete benefit schedule for medical and procedure case rates (including the exemptions) is provided in Annexes 1 and 2, and shall be posted in the PhilHealth website (www.philhealth.gov.ph).
IV. D. Computation of Reimbursement • When a patient has multiple conditions that are actively being managed during one confinement, the health care provider may claim for two case rates relevant to the conditions of the patient.
IV. D. Computation of Reimbursement • When a patient has multiple conditions … • The first case rate medical condition or procedure that used the most resources (drugs and medicines, laboratories and diagnostics, professional fees, etc) in managing the patient • The second case rate medical condition, or procedure with the second most resources used
IV. D. Computation of Reimbursement • When a patient has multiple conditions … • A case rate group shall not be allowed to be used both as first and second case rate in one claim except for procedures with laterality. Rules on procedures with laterality are found on item IV. G. 4.
IV. D. Computation of Reimbursement • When a patient has multiple conditions … • Initially, NOT all medical conditions or procedures may be claimed as second case rate. • A list of medical conditions, and procedures allowed as second case rate is provided in Annex 3. • Medical conditions and procedures not included in Annex 3 shall not be reimbursed as second case rate.
IV. D. Computation of Reimbursement • For a claim with a combination of case rates, the provider shall be paid the full case rate amount for the first case rate plus 50% of the second case rate. Combination: • medical condition and medical condition; • medical condition and procedure; or • procedure and procedure
MEDICAL CASE RATES If claimed as 1st Case Rate (100% of Case Rate) If claimed as 2nd Case Rate (50% of Case Rate) HCI Fee (20% of Case Rate) Professional Fee (30% of Case Rate) HCI Fee (70% of Case Rate) Professional Fee (30% of Case Rate) PROCEDURE CASE RATES If claimed as 1st Case Rate (100% of Case Rate) If claimed as 2nd Case Rate (50% of Case Rate) HCI Fee (10% of Case Rate) Professional Fee (40% of Case Rate) HCI Fee (fixed depending on RVU) Professional Fee (RVU x 56 x 1.5) Matrix of Payment for Combination of Case Rates
1st Case Rate (Medical): Subarachnoid haemorrhage from middle cerebral artery (ICD 10 Code: I60.1) (Case rate: 100% of P 38,000 = P 38,000) 2nd Case Rate (Medical): Acute subendocardial myocardial infarction (ICD 10 Code: I21.4) (Case Rate: 50% of 18,900 = P 9,450) Total Benefit = P 47,450 SAMPLECLAIM 1 Total Hospital Fee = P 30,380 Hospital Fee (70% of P 38,000 = P 26,600) Hospital Fee (20% of P 18,900 = P 3,780) Total Professional Fee = P 17,070 Professional Fee (30% of P 38,000 = P 11,400) Professional Fee (30% of P18,900 = P 5,670)
IV. D. Computation of Reimbursement • List of exemptions to the 50% rule on second case rate, which shall be paid in full even as second case rate:
Table 1. List of Exemptions to the 50% Rule on Second CaseRate
2nd Case Rate (Procedure): Hemodialysis (RVS Code: 90935) (Case Rate: 100% of 4,000 = P 4,000) Total Benefit = P 19,000 1st Case Rate (Medical): CAP III (ICD 10 Code: J18.92) (Case rate: 100% of P 15,000 = P 15,000) SAMPLE CLAIM 4 Hospital Fee (70% of P15,000 = P 10,500) Hospital Fee (Fixed P 3,500) Total Hospital Fee = P 14,000 Professional Fee (Fixed P 500 = P 500) Total Professional Fee = P 5,000 Professional Fee (30% of P 15,000 = P 4,500)
IV. D. Computation of Reimbursement • Aside from being exempted from the 50% rule, claims of multiple sessions of the following procedures under Procedure List A shall be reimbursed even if claimed as second case rate subject to other reimbursement rules.
IV. D. Computation of Reimbursement • Computation of reimbursements based on first & second CR (if applicable) as declared by the HCI in PhilHealth CF 2. The total benefit (sum of the first CR and 50% of the second CR) shall be deducted from the total actual charges (HCI fee + PF). The remaining amount shall be charged as out of pocket to the beneficiary except in cases where the NBB policy applies.
Table 2. Computation of Reimbursement and Multiple Sessions in One Claim
Table 3. Computation of Reimbursement for NBB, Multiple Sessions in One Claim NBB