Impact of Amniotomy, Oxytocin, and Epidural on Labor Duration and Birth Mode
10 likes | 124 Vues
This study examines how the timing of amniotomy, epidural anesthesia, and oxytocin affects labor duration and mode of birth among primiparae and multiparae. Utilizing a cohort from Lower Saxony, Germany, the research reveals that interventions during labor can significantly influence outcomes, such as increased caesarean section rates and altered labor progression. The analysis employs generalized Cox-regression models to account for various demographic and clinical factors, contributing valuable insights to clinical practice and guidelines for labor management.

Impact of Amniotomy, Oxytocin, and Epidural on Labor Duration and Birth Mode
E N D
Presentation Transcript
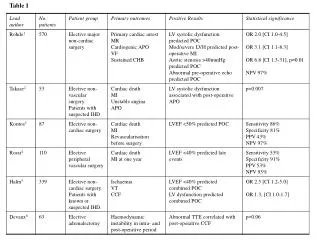
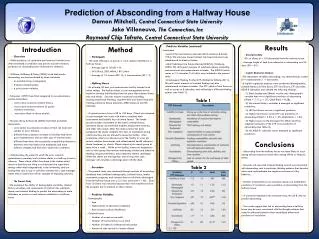
ID # 185245 Departement of Obstetrics, Gynaecology and Reproductive Medicine Departement of Biometry The timing of amniotomy, oxytocin and epidural and its association to labor duration and mode of birth Mechthild M. GROSS, Ph.D.¹, Hartmut HECKER, Professor², Cornelia FROEMKE, Ph.D.², Peter HILLEMANNS, Professor¹ ¹ Department of Obstetrics, Gynaecology and Reproductive Medicine, Hannover Medical School, Germany ² Department of Biometry, Hannover Medical School, Germany Introduction: Intrapartum interventions are intended to promote the progress of labor. Little is known about how the timing of amniotomy, epidural anesthesia and oxytocin impacts on the outcome of labor¹. The methodological challenges of examining labor progression have only recently been appreciated, especially in relation to clinical practice². The aim of the study is to investigate the associations between the timing of oxytocin, amniotomy, epidural analgesia as well as pre-existing time-constant factors on the duration and mode of birth. Results Primiparae: Results Multiparae: The onset of labor was defined as regular or irregular contractions in association with cervix dilation, and was identified by the attending midwife. Intrapartum time-varying factors were amniotomy, epidural analgesia, and oxytocin augmentation. The time dependence of these interventions was modeled as indicator functions, defined on an axis of time after onset of labor, switching from zero to one at the point in time of the intervention according to time to event analysis³. In time to event data, Kaplan Meier estimates were applied to allow for censoring. Duration of birth was studied for multiple, competing endpoints. These endpoints were full cervical dilation and caesarean section during first stage of labor as well as spontaneous or operative vaginal birth and caesarean section for the second stage. Demographic variables, antenatal care, risk status or induction method were constant in time, since for the individual woman the values of these variables did not change during the birth process (Tab. 1). Figure 1-2: Plotted graph of the effects of amniotomy, oxytocin and epidural on first stage duration and mode of birth. Effects are adjusted for confounders, see table 2 for detailed results. Figure 6-7: Plotted graph of the effects of amniotomy, oxytocin and epidural on first stage duration and mode of birth. Effects are adjusted for confounders, see table 2 for detailed results. Material and Methods: This state-wide cohort study focused on process-oriented care during childbirth in Lower Saxony, which is one of the German federal states. Pregnant women expecting a single vital fetus in vertex presentation and planning a vaginal birth after at least 34 completed weeks of gestation were eligible for the study. The sample consisted of 2090 primiparae (first birth) and 1873 multiparae. From the total sample of 3963 hospital births in 47 maternity units, 1169 forms were collected prospectively and 2794 retrospectively. Written informed consent was obtained from all patients in the prospective group before inclusion in the study. Institutional approval was granted by the ethics committee of Hannover Medical School and by the ethics committee for all public hospitals in Lower Saxony, Germany. Steps of multivariate data analysis for first and second stage: 1.Generalized Cox-regression model for each domain (demographic factors, risk-associated factors, child-related factors, induction), 2.Generalized Cox-regression model for all significant factors of step 1 and time-varying intrapartum factors (Results not shown), 3.Generalized Cox-regression model after backward selection (Tab. 2). Figure 3-5: Plotted graph of the effects of amniotomy, oxytocin and epidural on second stage duration and mode of birth. Effects are adjusted for confounders, see table 2 for detailed results. Figure 8-10: Plotted graph of the effects of amniotomy, oxytocin and epidural on second stage duration and mode of birth. Effects are adjusted for confounders, see table 2 for detailed results. Table 1: Description of variables Table 2: Generalized Cox-regression model after backward selection Primiparae: From amniotomy onwards first and second stage were accelerated. The rate for caesarean sections increased during first stage.Start of oxytocin augmentation was associated with an acceleration to both endpoints full dilation and caesarean section and increased the risk for an operative vaginal birth mode as well as the risk of a caesarean section. Primiparae with an epidural experienced an increased risk for a caesarean section during first stage. Epidural administration prolonged first stage before 7 hours after onset and accelerated after 7 hours till full dilation. Second stage was prolonged but primiparae had a decreased likelihood of operative vaginal birth during the first 11 hours of labor. Multiparae: The accelerating effect of an amniotomy decreased from a high to a medium level the longer the first stage duration continued. The risk for an operative vaginal birth was lower compared to those multiparae with spontaneous rupture of membranes and no amniotomy. Start of oxytocin augmentation was associated with acceleration to both endpoints full dilation and caesarean section during first stage and an increased risk for an operative vaginal birth mode during second stage. The later oxytocin augmentation was started the more likely spontaneous birth was delayed. The later an epidural was performed, the less likely a spontaneous birth and the more likely a caesarean section. Conclusion: Effects of amniotomy, oxytocin and epidural differ during the process of birth and consequently with duration and mode of birth. In primiparae, an epidural between 7 and 11 hours of birth duration may prevent from dysfunctional labor. Financial support: The study was funded by the Deutsche Forschungsgemeinschaft (German Research Council) References: 1. Wong CA, Scavone BM, Peaceman AM, et al. The Risk of Cesarean Delivery with Neuraxial Analgesia Given Early versus Late in Labor. N Engl J Med 2005; 352:655-65 2. Vahratian A, Troendle JF, Siega-Riez AM, Zhang J. Methodological challenges in studying labour progression in contemporary practice. Paediatri Perinat Epidemiol. 2006; 20(1):72-8 3. Smith GCS, Pell JP. Use of time to event analysis to estimate the normal duration of human pregnancyy. Hum Reprod 2001; 16: 1497-500 1 No. of Pp/Mp: 2090/1872,2 No. of Pp/Mp: birth weight: 2089/1872; length: 2087/1872; head circumference: 2086/1869; sex: 2088/1872, 3 administered before onset of labor, 4administered at/after onset of labor, 5 593/109 censored due to operative vaginal delivery or caesarean section (Kaplan-Meier; Pp/Mp: 2090/1873). Cases with negative or missing times are ignored,6 593/109 censored due to caesarean section (Kaplan-Meier; Pp/Mp: 2090/1870). Cases with negative or missing times are ignored, 7 297/47 censored due to operative vaginal delivery or caesarean section (Kaplan-Meier; Pp/Mp: 1794/1808). Cases with negative or missing times are ignored. Contact: Dr. Mechthild M. Gross, Department of Obstetrics, Gynaecology & Reproductive Medicine, Hannover Medical School, Carl-Neuberg-Str. 1, D-30625 Hannover, Germany, Phone: ++49-511-532-6116, Fax: ++49-511-532-6191, Email: Gross.Mechthild@mh-hannover.de