Download
1 / 30
300 likes | 329 Vues
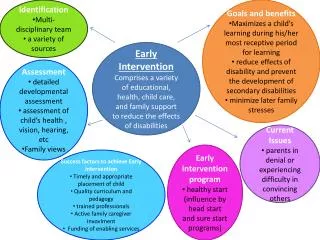
Explore the Connecticut Birth to Three program focusing on early identification, team approach, and family-centered services for children with hearing loss. Learn about comprehensive intervention principles and supportive resources.

E N D
Early Intervention Applications: Connecticut Guidelines Antonia Brancia Maxon, Ph.D., CCC-A1, 2 Linda Goodman, M.A., M.P.A. 2 Lynn Skene Johnson, M.S. 2 1 New England Center for Hearing Rehabilitation Hampton, CT 2 Connecticut Birth to Three Program Hartford, CT
Faculty Disclosure InformationIn the past 12 months, we have not had a significant financial interest or other relationship with the manufacturer of the product or provider of the services that will be discussed in our presentation.This presentation will not include discussion of pharmaceuticals or devices that have not been approved by the FDA.
Connecticut Birth to Three Mission • Strengthen the capacity of Connecticut’s families to meet the developmental and health-related needs of their infants and toddlers who have delays or disabilities. • The system ensures that all families have equal access to a coordinated program of comprehensive services and supports. CT Guidelines 2005
Connecticut Birth to Three Mission • Ensure that all families have equal access to services and supports that: • foster collaborative partnerships; • are family centered; • occur in natural settings; • recognize current best practices in early intervention; and • are built on mutual respect and choice CT Guidelines 2005
Part C Implementation: Connecticut • The Connecticut Birth to Three System provides comprehensive services to children with a wide range of disabilities and delays and their families through a network of approved programs. • Implementation of Part C for infants and toddlers with hearing loss in Connecticut is conducted in a unique way. • Three state-wide specialty programs have specific expertise in working with children who are hard of hearing or deaf and their families. CT Guidelines 2005
Connecticut Part C Program for I/T With Hearing Loss • Three statewide programs that specialize in working with children who are hard of hearing or deaf • Serve children living in any town in Connecticut • Families may choose the program most compatible with their desired outcomes regardless of geographic location • Families may also choose one of the comprehensive programs CT Guidelines 2005
Connecticut Part C Program for I/T With Hearing Loss • Guidelines for Infants and Toddlers Who are Deaf or Hard of Hearing • developed by an interdisciplinary group of professionals and parents in 1999 • revised in 2005 • assists families in understanding their child’s hearing loss • ensures that families are aware of the services that are appropriate and necessary for their children • organized according to 8 principles
Intervention: Principle 1 • Early identification and diagnosis is essential • Behavioral characteristics of children who are hard of hearing or deaf • presented to help with hearing loss identification for young children who have late-onset, progressive or acquire a hearing loss CT Guidelines 2005
Intervention: Principle 2 • Ongoing audiological assessment and management must be conducted by professionals trained to work with infants and young children. • Professionals involved in hearing management • Pediatricians • ENTs • Audiologists • Hearing aid dispensers CT Guidelines 2005
Intervention: Principle 2 (cont’d) Trained professionals (cont’d) • What to expect from a pediatric audiologist • 14 criteria described to help parents make choices • Descriptions of tests used by pediatric audiologist • Auditory Brainstem Response • Otoacoustic Emissions • Immittance Measures • Behavioral Observation Audiometry • Visual Reinforcement Audiometry • Conditioned Play Audiometry CT Guidelines 2005
Intervention: Principle 3 • The intervention team should assist the family in learning about the nature of their child’s hearing loss. • Descriptions of the parts of the ear • Descriptions of different types of hearing loss • Conductive • Sensorineural • Mixed • Auditory Neuropathy • Unilateral CT Guidelines 2005
Intervention: Principle 4 • Intervention requires a team approach. • The family is the most important member of this team. • The Birth to Three System offers support, assistance, and advice to families on how to best meet their child’s unique needs. • This should include access to a wide variety of information that is shared in an unbiased manner. • Communication modality • Use of amplification • CI candidacy CT Guidelines 2005
Intervention: Principle 4 (cont’d) Intervention requires a team approach (cont’d). • components of family training • components of parent support services • listing of potential members of the intervention team • Audiologist • Auditory-Verbal Therapist • Speech-Language Pathologist • Special Education Teacher • Teacher of the Hearing Impaired • Others • Medical professionals CT Guidelines 2005
Intervention: Principle 5 • Parents and children are partners in communication and must develop a communication system in order for a language system to develop. • communication approaches and options • Auditory-Oral/Auditory Verbal • Cued Speech • Total Communication CT Guidelines 2005
Intervention: Principle 6 • Language development begins as soon as a child is born and develops through interactions with the family during daily routines. • Families understand aspects of language development • Children and families need a way to communicate with one another • Children need daily opportunities to learn and use language in natural settings CT Guidelines 2005
Intervention: Principle 7 • Parents need to understand and manage the hearing aids and/or auditory equipment for their child. A program must help the family learn how to maintain any hearing aids or equipment. • Understanding initial and ongoing needs • “Work in Progress” • Understanding what assistive technology is needed and how it works CT Guidelines 2005
Intervention: Principle 8 • Parents are advocates for their children who are hard of hearing or deaf. Early intervention should help parents understand their rights as identified in state and federal legislation. • IDEA (Parts B and C) • Section 504 • Americans with Disabilities Act CT Guidelines 2005
Transitioning From Part C Services • Transition from B23 to Preschool/Part B • transition plan included in all IFSPs • referral to school district by 24 months • transition conference at least 90 days and up to 9 months before 3rd birthday • Parents need to be knowledgeable about Part B eligibility and programming • Things parents should consider as part of transition from Birth to Three services
Transitioning From Part C Services • Things parents should consider as part of transition from Birth to Three services to LEA • the child’s continued need for audiological services; • assistance with acquiring and maintaining any assistive technology the child currently uses; • communication modality (access to language in the modality the family has chosen);
Transition Considerations(cont’d) • who the family will contact for ongoing information and guidance with the child’s hearing impairment; • interaction with peers including children who are and are not hard of hearing or deaf; • transportation; • any additional need for equipment; • the classroom environment including the acoustics of the setting;
Things to consider • the philosophy of the school program; • staffing; • training needs for staff; and • levels of support needed. The PPT (including parents) reviews developmental information to determine eligibility.
Questions and Answers A series of frequently asked questions posed by parents with answers. Some examples: Q: My child’s audiologist has not been able to complete an audiogram on my child, yet she wants him to wear hearing aids. Is that OK? A: Yes, the identification of a child with a hearing loss is the first step in the process of audiological services. When a child is very young, it may take a series of evaluations to complete a hearing profile. At the same time, the audiologist should put hearing aids on the child as soon as possible and refine them over time. A pediatric audiologist will use the information acquired in testing as well as in trial periods with hearing aids to complete the audiological recommendations for your child.
Questions and Answers Q: How do I know if my son is a candidate for a cochlear implant? A: This is a discussion you will need to have with a variety of people, including your son’s primary health care provider, audiologist, and intervention team. This decision will be made based on the extent of your son’s hearing loss, the benefit he gets from wearing hearing aids, and an evaluation performed at a cochlear implant center. Your son’s service coordinator can provide you with information and resources about this process.
Appendices and Index • Mission of the Connecticut Birth to Three System • Types of Hearing Tests • Description of and Audiogram • Resources Available on the Internet, Connecticut Resources and National Resources • What is Relay Service?
Specialty Programs • In Connecticut infants and toddlers who are hard of hearing or deaf can receive services through one of the three specialty programs. • American School for the Deaf • New England Center for Hearing Rehabilitation • Soundbridge
Specialty Programs • Benefits • Service coordinators have expertise in hearing loss and its associated developmental effects • Audiologists part of the program • Staff knowledgeable about needs of I/Ts with hearing loss and their families • Staff knowledgeable about assistive technology • Staff knowledgeable about the child’s needs in preschool – the transition process • Staff knowledgeable about IFSP components for I/Ts with hearing loss
Specialty Programs • Difficulties • Statewide travel • Incorporating other services • Intensity of services
Assistive Technology • B23 payer of last resort for assistive technology • Request for funding pending insurance payments • All assistive technology and supplies are ultimately funded (after approval) • significantly reduces delay in providing amplification, earmolds, supplies • audiologists are willing to move forward with amplification
Unique Needs of Infants and Toddlers with Hearing Loss • Connecticut’s Part C implementation recognizes the unique needs of infants and toddlers with hearing loss and their families • Audiological management and assistive technology are included as a service in the child’s Individualized Family Service Plan (IFSP). • recognizes that auditory development is basic to communication regardless of modality
Connecticut’s Service Provision Model • This model of service provision recognizes that all infants and toddlers with hearing loss need intensive services. • Children who need other services (e.g., PT) will have them included in the IFSP. • As the professionals have expertise in hearing loss all early intervention services can be provided in a family-centered, supportive approach that addresses the specific associated needs. • Families are not required to select one of the three specialty programs. They may opt for one of the comprehensive programs.