Download
1 / 42
560 likes | 1.85k Vues
Principles and Application of Flow Cytometry. Rodney Stuart, MD August 5,2005. Objectives. Basic principles of flow cytometry Separation of cells on appearance Separation based on light emitting dyes Eliminating bleed over between colors Studying the cells of interest

E N D
Principles and Application of Flow Cytometry Rodney Stuart, MD August 5,2005
Objectives • Basic principles of flow cytometry • Separation of cells on appearance • Separation based on light emitting dyes • Eliminating bleed over between colors • Studying the cells of interest • Examples of difficult cases
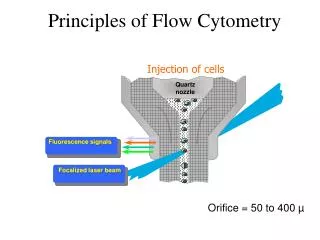
Flow Cytometry • First labeled with fluorescent dyes. • Forced through a nozzle in a single-cell stream passing through a laser beam • The laser is focused to a known wavelength • Excitation of a specific fluorochrome • Photo-multiplier tubes detect the scattering of light and emission from the fluorescent dye
Forward Scatter • Cells pass through a small (50-300 µm) orifice • Detection ranges from 0.5-40 µm • the amount of light scattered in the forward direction (along the same axis that the laser light is traveling) = size of cell
Side Scatter • the amount of light scattered to the side (perpendicular to the axis that the laser light is traveling) is detected in the side or 90o scatter channel • Equates to shape and homogeneity of cells (AKA-granularity/complexity)
Neutrophils Monocytes Forward Scatter (Size) Lymphocytes Side Scatter (granularity) Forward and Side Scatter
Fluorescence Channels • The specificity of detection is controlled by the wavelength selectivity of optical filters and mirrors
PE-Texas Red Propidium Iodem FITC ECFP EGFP EYFP PE-Cy5 APC PerCP PE DsRED FL1 ~525nm FL2 ~575 nm FL3 ~620 nm FL4 ~675 nm Fluorochromes
One Parameter Histogram • A one-parameter histogram is a graph of cell count on the y-axis and the measurement parameter on x-axis. Events FITC
-/+ +/+ -/- +/- Two Parameter Histograms • A graph representing two measurement parameters, on the x- and y-axes, and cell count height on a density gradient. This is similar to a topographical map.
PE-Texas Red Propidium Iodem FITC ECFP EGFP EYFP PE-Cy5 APC PerCP PE DsRED FL1 ~525nm FL2 ~575 nm FL3 ~620 nm FL4 ~675 nm FL1 ~525nm FL2 ~575 nm FL3 ~620 nm FL4 ~675 nm Compensation • The inherent overlap of emission spectra from antibody fluorescent labels makes compensation necessary. • Use a negative control to set your High Voltages (HV) per detector. As a rule of thumb set the High Voltages so that your negatives are in the 1st decade of the parameters being collected. Lower high voltage settings will also result in lower compensation settings.
Compensation • The amount of spectral overlap is corrected by subtracting a percentage from the total of FL1 fluorochrome pulse generated by the FL1 detector. The FL1 fluorochrome “spillover” detected by the FL2 detector can be viewed as interference. By subtracting a percentage of the total FL1 fluorochrome pulse from the total pulse generated by the FL2 detector (eg. PE + FITC interference) you can obtain a FL2 fluorochrome only pulse. • Running samples that are individually stained with the antibody-fluorochrome components of your multi-color samples aids in appropriate compensation.
FITC PE Compensation FL1 = FL1 - %FL2 compensation slider
-/+ +/+ -/- +/- Compensation -/+ +/+ -/- +/-
Neutrophils Monocytes Forward Scatter (Size) Lymphocytes Side Scatter (granularity) Gating • Allow you to view cells of interest • lets you decide which data to view and which data to ignore or discard. • Gating can subsequently be changed when you analyze your data without any loss of information.
Case Scenarios Non-Hodgkin B cell Lymphoma/Leukemia
Case 1 • 31 year-old African American HIV+ male who presents with a rapidly enlarging neck mass
Follicular Lymphoma(FL) • Most common NHL in the Western World (45% of adult lymphomas) • Middle age distribution affecting males and female equally • Morphology: partial or often complete nodal architectural effacement by numerous closely packed follicular nodules that most frequently homogenous with numerous small cleaved follicular center cells/centrocytes and larger cells with open nuclear chromatin, several nucleoli, and modest amounts of cytoplasm, referred to as centroblasts • Bone marrow involvement in 85% of patients (paratrabecular)
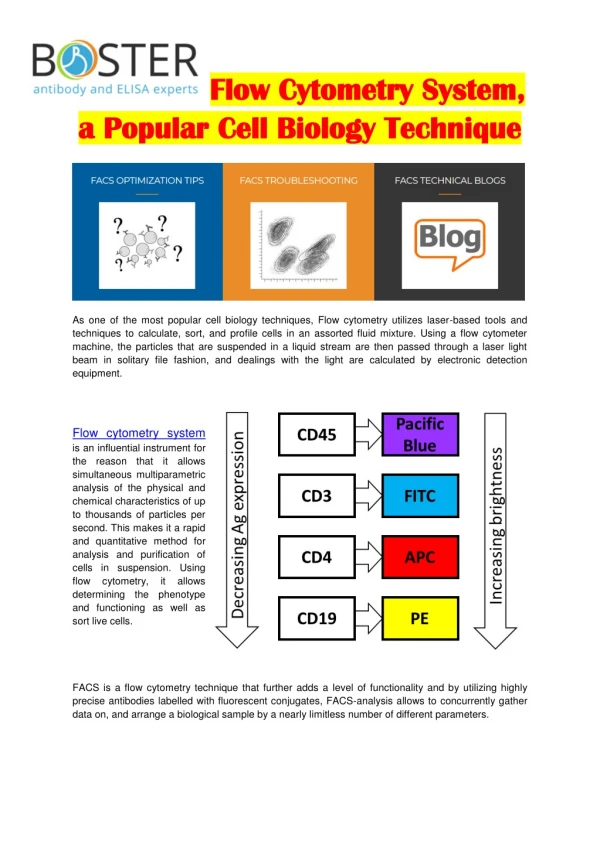
Immunophenotyping • Strong CD19, CD20 • Monotypic immunoglobulin or no surface Ig expression • CD10 positive • Negative for CD5 and CD43
Diffuse Large B-cell(DLBCL) • 20% of NHL • Median age of 60 years with a male predominance • However age range is wide (5% of childhood lymphoma) • 4 variants: centroblastic, immunoblastic, T-cell/histocyte-rich, and anaplastic • Morphology: diffuse large lymphoid cells (4-5X the size of small lymphocytes)with vesicular chromatin. Nuclear features can range from multilobated, cleaved, or even the appearance of Reed-Sternberg cells
Immunophenotyping • CD20 and CD19 seen in many but not all • More common than FL to be sIg negative • Some contain cytoplasmic Ig • Some mark like FL (CD5-, CD10+,bcl-6+, bcl-2+) but can lack CD10, bcl-6, and bcl-2
Burkitt Lymphoma (BL) • Rapidly dividing transformed cell lymphoma • Adolescents or young adults • Follicular formation in a minority of cases • Morphology: Diffuse infiltrate of intermediate-sized lymphoid cells. • Round or oval nuclei with course chromatin, several nucleoli, and basophilic or amphophilic cytoplasm • “Starry sky” appearance due to presence of numerous tingible-body macrophages
Immunophenotyping • CD19, CD20+ • CD10+ • BCL6+ • Express monotypic light chains • Cytoplasmic Ig may be present • CD5-
Cytogenetics • Follicular Lymphoma: t(14;18) (Ig-H and bcl-2 gene) (90% of FL) • Diffuse Large B cell Lymphoma: variable, many with translocations involving chromosome 3q27 (BCL6 locus), 10-20% contain t(14;18) • Burkitt Lymphoma: c-myc associated t(8;14), t(8;22), t(2;8)
Case 2 • 58 year old Caucasian male initially presented with fatigability, weight loss, and anorexia. He was found to have CLL and is currently on chemotherapy.
Small Lymphocytic Lymphoma/Chronic Lymphocytic Leukemia • CLL: Most common Leukemia in adults in the Western world • SLL: 4% of NHL • Older adults • Morphology: population of small lymphocytes containing round to slightly irregular nuclei with condensed chromatin and scant cytoplasm, mixed with larger prolymphocytes • Smudge cell on peripheral smear
Immunophenotype • CD19 and CD20+ • CD23 and CD5+ • Low level expression of sIg and monotypic light chain
Rituximab • anti-CD20 monoclonal antibody • Rituxan may induce antibody-dependent cell-mediated cytotoxicity • Rituxan may also induce complement-dependent cytotoxicity • Causes decrease in CD20 available for detection ab to bind • Either through direct binding site competition • Or transient down-regulation of CD20
Case 3 14 year-old Caucasian male with previously diagnosed lymphoid neoplasm for which he was treated with chemotherapy. He has been clinically asymptomatic with close follow-up for the last year. Current bone marrow biopsy obtained is shown here:
Acute Lymphoblastic Leukemia (ALL) • Consists of immature, pre-cursor B (Pre-B) (85%) or T (Pre-T) lymphocytes • Pre-B manifests in childhood (many subtypes by European Group for the Immunological Characterization of Leukemias) • Pre-T manifests in adolescents • Morphologically indistinguishable • Immunophenotyping needed for typing
ALL Immunophenotyping • Terminal deoxynucleotidyl transferase (TdT) + >95% of time • Pre-B • Positive for: CD19, CD22, CD79a, CD24, CD34, CD45, HLADR, CD38, CD9, and CD10 • Negative for: surface Ig expression • Pre-T • Positive for: CD1, CD2, CD5, CD7
Hematogones • Bone marrow B-cell precursors (detected on flow in 80% of bone marrow aspirates) • Cytologic features: • Size: 10-20 microns • May appear as mature lymphocytes • Small cell with round or oval nucleus • May be indistinguishable from neoplastic lymphoblasts • Sometimes exhibits 1 or more indentations or shallow clefts with condensed chromatin • Rim of deeply basophilic cytoplasm
Hematogones • Most numerous in children (up to 21%) of bone marrow in infants and declines to <5% after 16 • Have been observed in reactive lymph nodes and in peripheral blood • Usually TdT negative • Other conditions can increase the number in adults • Regenerating marrow following chemotherapy • Autoimmune diseases • Congenital cytopenias • Lymphomas (usually stage 3) • Neuroblastomas • AIDS
Hematogone Immunophenotype • Always positive for: • Progenitor cell markers CD34 and CD38 • CD19 • Dim CD22
Hematogone Immunophenotype • Maturation markers: • Stage 1(red): • Positive TdT and Bright CD10 • Stage 2(blue): • Moderate CD10, dim CD20, and variable sIG • Stage 3(Yellow): • Dim to moderate CD10, moderate to bright CD20, and variable sIG
Hematogones vs. ALL Red=Lymphoblasts Yellow=Hematogones Concurrent CD34 and CD20 Abberant over-expression of markers (eg. CD10)
References • http://biology.berkeley.edu/crl/flow_cytometry_basic.html • Gervasi F, Lo Verso R, Giambanco C, Cardinale G, Tomaselli C, Pagnucco G. Flow cytometric immunophenotyping analysis of patterns of antigen expression in non-Hodgkin's B cell lymphoma in samples obtained from different anatomic sites.Ann N Y Acad Sci. 2004 Dec;1028:457-62. • Kroft SH, Asplund SL, McKenna RW, Karandikar NJ.Haematogones in the peripheral blood of adults: a four-colour flow cytometry study of 102 patients.Br J Haematol. 2004 Jul;126(2):209-12. • S Sava an1, M Büyükavc 2, S Buck1 and Y Ravindranath1 . Leukaemia/lymphoma cell microparticles in childhood mature B cell neoplasms. Journal of Clinical Pathology 2004;57:651-653. • Maloum K, Sutton L, Baudet S, Laurent C, Bonnemye P, Magnac C, Merle-Beral H.Novel flow-cytometric analysis based on BCD5+ subpopulations for the evaluation of minimal residual disease in chronic lymphocytic leukaemia.Br J Haematol. 2002 Dec;119(4):970-5. • Jilani I, O'Brien S, Manshuri T, Thomas DA, Thomazy VA, Imam M, Naeem S, Verstovsek S, Kantarjian H, Giles F, Keating M, Albitar M.Transient down-modulation of CD20 by rituximab in patients with chronic lymphocytic leukemia.Blood. 2003 Nov 15;102(10):3514-20. Epub 2003 Jul 31