Download

1 / 30
300 likes | 484 Vues
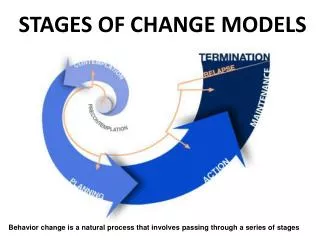
Designing for Behavior Change in Agriculture, Natural Resource Management, Health & Nutrition Tom Davis Senior Specialist, SBC (TOPS). How this Session Differs from Earlier TOPS Training DBC Session.

E N D
Designing for Behavior Change in Agriculture, Natural Resource Management, Health & Nutrition Tom Davis Senior Specialist, SBC (TOPS)
How this Session Differs from Earlier TOPS Training DBC Session • Essentially repeating the session for the sake of FSN Network participants who were not here Monday and Tuesday • More Health/Nutrition vs. ANR focus • 1.5 vs. 2.0 hr session
Designing for Behavior Change Training • A practical behavioral framework that aids food security implementers in planning their projects strategically for maximum effectiveness. • 5.5 day course for Ag, NRM, Health and Nutrition staff • TOPS co-hosted DBC regional trainings in Niger (August 2011), Ethiopia (Fall 2011), and Asia (Spring 2011), plus nine country-level trainings. Contact Tom Davis (tdavis@fh.org) if interested in hosting the DBC training in your country.
Session Objectives • Participants will be able to: • State advantages of using DBC to plan their ANR activities and messages; • Understand the DBC framework; • Cite the three most powerful determinants of behavior measured in Barrier Analysis (little focus on other determinants); • List the seven steps in Barrier Analysis; • Explain how to collect BA data; • Explain how to analyze Barrier Analysis data; • Explain how to use BA data. • Not a full DBC training (takes 5.5 days)
Recent Modifications in DBC Training Manual • Changed from all health/nutrition examples to 2/3 ANR and 1/3 Health/Nutrition examples. Still plenty of H/N examples, training stories, etc. • Modified descriptions and presentation of behavioral determinants (but essentially the same) • Some changes to analysis of Barrier Analysis data (analysis is done using an Excel tabulation table) • More ANR training activities (e.g., teaching stories, ANR DBC frameworks).
Why Behavior Change is Central Development in all sectors requires that people do something new/different. Nothing particular about health sector behavior change. You can find methods/tools (health, psychology, marketing / business) and modify for your purposes. When examining methods/tools, look for a link to the scientific literature. A great place to start: Designing for Behavior Change
What works in behavior change?Findings from Powerful to Change Studies CORE SBCWG compared low and high performers for several behaviors (e.g., exclusive BF, hand washing with soap) – what works in changing behavior? Using formative research (e.g., Barrier Analysis, positive deviance studies, Trials of Improved Practices) especially to find the determinants of behaviors and to choose the right messages/activities; and Using the right coverage strategy: Using systematic home visitation (through cascade training like Care Groups) to reach more people more often.
Example of Using Formative Researchin Ag/NRM: DBC in Guatemala CRS’ SEGAMAYA program, two different provinces of Guatemala: San Marcos and Baja Verapaz (culturally similar) June 2009: Staff in one San Marcos received Designing for Behavior Change training, did Doer/NonDoer Analysis (a short version of Barrier Analysis), developed a DBC strategy and indicators for Ag/NRM. Planned to replicate in the Baja Verapaz area, but were too busy responding to an emergency in another area. Same program and monitoring system in both areas, so Baja Verapaz served as comparison area to examine results of the DBC training/strategy.
San Marcos, Guatemala: Use of Designing for Behavior Change Decided to study key soil conservation practices. “Planting ‘live barriers’ along the edges of planting terraces” identified as the practice with the lowest adoption rate, despite requiring only labor and local, free plant material. San Marcos area: Participated in a Designing for Behavior Change (DBC) Workshop and Conducted a Barrier Analysis Survey. In comparison area -- Baja Verapaz -- determined strategy and messaging using their past experiences in the area, etc. (No formative research.) Found that: (1) most farmers fully understood the benefits of the practice, (2) Doers worked together to plant the barriers, and (3) Doers liked practice because they did not lose plantings due to drought. San Marcos Strategy focused on organizing farmers to work together on each other’s land during the off-season to plant the barriers. Farmers groups brainstormed to develop strategies to prevent loss of plants due to drought.
Results: Number of Hectares Planted with Live Barriers Used DBC Did not use DBC
Focus Group Comments To staff: Overall, was the (DBC) training and development of a BC strategy helpful? “Yes, this completely changed our way of thinking. We no longer think in terms of “we” and “them”, rather we are a team with the participants in finding solutions to the barriers.” “It never occurred to us before [the training] to figure out the barriers or what makes people want to change. We wasted so much time and energy repeating the benefits over and over, then, feeling frustrated because no one adopted the new practices.” What was the most useful part of the (DBC) training? “Going to the field to do the Doer/Non-doer Surveys. Until we saw those responses, we thought we knew our target farmers and what they think. It was incredibly revealing.” “Understanding the wide range of factors [determinants] that influence adoption of practices.”
Decrease in Malnutrition 42% decrease in underweight in 31 months All districts were at or above project target for EBF.
Overview of the Designing for Behavior Change Framework See Blank Framework and DBC Framework for Penning Chickens handouts
Important Determinants that Influence Behavior • See Handout • These Three Most Powerful Determinants should always be explored: • Perceived Self-efficacy/Skills (control beliefs): Individual's belief that s/he can do a particular behavior given their current knowledge and skills. Includes what makes it easier and what makes it more difficult. • Perceived Social Norms: Perception that people important to an individual think that s/he should do the behavior. Includes who approves/disapproves. • Perceived Positive or Negative Consequences: What a person thinks will happen, either positive or negative, as a result of performing a behavior. Includes advantages /disadvantages of the behavior. • (Other determinants are listed in the handout.)
The Barrier Analysis Process: Use the Results Tabulate and Organize the Results 7 Collect Field Data Results 6 Organize the Analysis Sessions 5 Develop Questions about Determinants 4 Develop the Behavior Questions 3 Define the Goal, Behavior and Target Group 2 Seven Steps in Barrier Analysis 1
Step 1: Defining the Goal, Behavior and Priority Group • Example: Antenatal Care • What exactly do you want to promote (the behavior)? Who do you want to do it (the priority group)? To what extent do you want them to do it (the goal)? • Priority Group (who): Pregnant women and mothers of infants. • Behavior: Going for at least 4 antenatal care visits. • Goal statement: All pregnant women will go for at least four antenatal care visits.
Low Perceived Susceptibility The Problem?? “AIDS is mostly transmitted by heterosexual sex” “I know how to use condoms” “My friends approve” “My boy/girlfriend will stay with me…”
“AIDS is mostly transmitted by hetero-sexual sex” “I know how to use condoms” “My friends approve” “My boy/girlfriend will stay with me…” AIDSCOM, Eastern Caribbean, 1991
Step #2: Develop the Behavior Question See Antenatal Care Questionnaire (Questions #1, #2 and gray box.)
Step #3: Develop Questions on Each Determinant See rest of questionnaire with questions on each determinant.
Step #4, Organize Analysis Sessions & Step #5, Collect Field Data • Step #4: Choose the communities / areas where you will interview 90 people. Choose from a larger area, for example, 9 randomly-selected communities x 5 Doers & 5 NonDoers from each). Little time available? Then 5 communities x 9 Doers and 9 NonDoers each. • Step #5: Use the questionnaire to interview 45 Doers and 45 NonDoers per study. Study one key behavior per study. (Enough respondents to generate useful project planning data while not identifying small, less important differences).
Step #6: Tabulating and Analyzing the Results • Tabulate the questionnaire data on newsprint. • Analyze the Results using Excel: See next slides on interpretation.
Interpreting BA Data When Doers and Non-Doers have similar percentages for any item Item is not a likely determinant of the behavior. When Doers’ and Non-Doers have very dissimilar percentages for any item Item is very likely to be an important determinant of the behavior. Look for differences where p < 0.05 – that is, the probability that a difference is due to chance is less than 5%. Larger Odds Ratio More important determinant.
Interpreting BA Data Doers’ responses may include ideas for strategies on how to make the behavior easier or more appealing, and could provide clues for messages to Non-Doers. Examine these carefully. Sometimes more Doers list a particular disadvantage of the behavior than do Non-Doers. Looking at differences between Doers and Non-Doers as to who approves or disapproves of the behavior may provide important information on who to target for your intervention.
Step #7: Use the Results • See “Linking Determinants with Activities” handout (focus on Self-efficacy/Skills, Perceived Social Norms, and Positive/Negative Consequences)
Step #7: Use the Results • Small Group Work: Use handout on Antenatal Care BA study to come up with at least twoactivities (not messages) that respond to the determinants that your group is examining: • Group A: Focus on Perceived Positive Consequences • Group B: Focus on Perceived Negative Consequences • Group C: Focus on Perceived Barriers and Enablers – What makes it Easier, What makes it Difficult • Group D: Focus on Social Norms – Who Approves / Disapproves. • ONLY FOCUS ON IMPORTANT DETERMINANTS (p<0.05) • ONLY ONE GROUP WILL REPORT OUT (but I’ll check all work)
Other Resources • List of Social & Behavioral Change Key Competencies (handout) • Community Development Worker Quality Improvement and Verification Checklist (training session later this week) • List of FSN Network SBC Task Force Approved Methods and Tools Take advantage of the full 5 ½ day DBC Training when it is offered in your country or region!
This presentation was made possible by the generous support of the American people through the United States Agency for International Development (USAID). The contents are the responsibility of Save the Children and do not necessarily reflect the views of USAID or the United States Government.