Understanding a 3-Year-Old's Recurrent Infections: Potential Immunological Causes
This case study explores the immunological challenges faced by a 3-year-old boy with recurrent bacterial and viral infections. He has a history of responding well to passive immunization but not to active immunization with non-virulent bacteria. Despite normal leukocyte phagocytic ability and digestion, the child's condition raises questions about possible underlying causes such as inactive CD8+ T cells, inability to produce antibodies, or incomplete MHC molecules. Additionally, implications of Bare Lymphocyte Syndrome (BLS) are discussed, highlighting the necessity for further investigation into his immune response.

Understanding a 3-Year-Old's Recurrent Infections: Potential Immunological Causes
E N D
Presentation Transcript
My name is _____ and I’m a 3-year old boy. I came into the ER with yet another bacterial infection. History: I have a history of repeated bacterial and viral infections. Passive immunization with antibodies was always successful, but active immunization with non-virulent bacteria always failed. Physical examination: I’m short for my age. Tests: My complete blood count was normal. More specific assays were done, for example, my leukocyte ability to phagocytose bacteria was normal, and the phagocytosed bacteria were digested normally. • What would you consider might be the cause of my condition? • Inactive cytotoxic CD8+ T cells • Inability to make antibodies • Inability to destroy antibody-coated bacteria • Incomplete major histocompatibility molecules (MHC)
Adaptive (acquired) immunity << Who is this?
Ag WHITEBOARD
My name is _____ and I’m a 3-year old boy. I came into the ER with yet another bacterial infection. History: I have a history of repeated bacterial and viral infections. Passive immunization with antibodies was always successful, but active immunization with non-virulent bacteria always failed. Physical examination: I’m short for my age. Tests: My complete blood count was normal. More specific assays were done, for example, my leukocyte ability to phagocytose bacteria was normal, and the phagocytosed bacteria were digested normally. • What would you consider might be the cause of my condition? • Inactive cytotoxic CD8+ T cells • Inability to make antibodies • Inability to destroy antibody-coated bacteria • Incomplete major histocompatibility molecules (MHC)
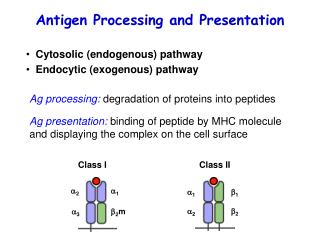
Bare lymphocyte syndrome (BLS) • Rare genetic disorder. • Leukocyte cells develop normally, but lymphocyte activity lacks. • This syndrome stems from inexpression of MHC class II, caused by the absence of one of several transcription factors required for expression of MHC class II. • These proteins include: • Class II trans-activator (CIITA) • Regulatory factor of the X box 5 (RFX5) • RFX-associated protein (RFXAP) • RFX ankyrin repeats (RFXANK; also known as RFXB) • Inactive cytotoxic CD8+ T cells • Inability to make antibodies • Inability to destroy antibody-coated bacteria • Incomplete major histocompatibility molecules (MHC) • What would you consider might be the cause of my condition? • Inactive cytotoxic CD8+ T cells • Inability to make antibodies • Inability to destroy antibody-coated bacteria • Incomplete major histocompatibility molecules (MHC)
My name is _____ and I was infected intranasally with flu virus. The virus attacked my nasal epithelial cells. Now, my sensitized cytotoxic CD8 lymphocytes aim to kill these virus-infected nasal epithelial cells. Their receptors recognize foreign proteins on the epithelial surface in association with: A. MHC class I heavy chain only B. MHC class I heavy chain and b2-microgIobulin C. MHC class I heavy chain and lgG D. MHC class II alpha-chain and beta-chain E. MHC class II alpha-chain only
My name is ______ and I joined a clinical trial in which I received a substance that prevented the acidification of lysosomes within my antigen-presenting cells. As a result, my affected cells showed impaired interaction with lymphocytes upon antigen exposure. The observed effect most likely results from a low cell surface expression of which of the following molecules? A. MHC Class I B. MHC Class II C. T-cell receptor D. Cytokine receptors
Homework: List the important HLAs in human autoimmune diseases For example HLA-DQ2 => Celiac