Download
1 / 38
390 likes | 753 Vues
Testing Source Plasma for Hepatitis B Virus by Nucleic Acid Testing. Blood Products Advisory Committee Meeting April 28, 2011 Susan A. Zullo, Ph.D. FDA/CBER/OBRR/DETTD. Presentation Outline. Issue Background Potential Benefits Product Safety Public Health Questions for the Committee.

E N D
Testing Source Plasma for Hepatitis B Virus byNucleic Acid Testing Blood Products Advisory Committee Meeting April 28, 2011 Susan A. Zullo, Ph.D. FDA/CBER/OBRR/DETTD
Presentation Outline • Issue • Background • Potential Benefits • Product Safety • Public Health • Questions for the Committee
BPAC Issue April 2011 • FDA seeks advice from the Committee on whether scientific data support the concept that testing Source Plasma for hepatitis B virus (HBV) DNA by nucleic acid testing (NAT) increases the margin of safety of plasma derivatives and whether such testing in donors adds to public health.
BPAC Issue April 2009 • FDA sought advice from the Committee on issues related to Whole Blood donor screening for HBV DNA by HBV NAT to prevent transfusion transmission of HBV. The Committee supported routine HBV NAT and establishment of a minimum sensitivity for individual samples.
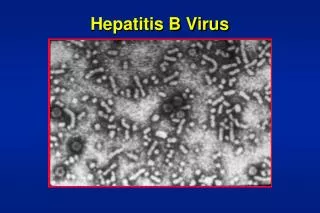
HBV Structure Enveloped DNA Virus
Morphology of HBV Non-Infectious 22 nm Sphere Non-Infectious Filaments Dane Particle/Infectious Virion
Hepatitis B Infection • Transmission through contact with infected blood or other body fluids (e.g. - sexual contact, IV drug use, mother to child during delivery) • 4,033 acute, symptomatic cases reported in the U.S. (2008) • Incidence of 1.3 cases per 100,000 • Estimated 800,000 – 1.4 million individuals with chronic HBV infection in the U.S. resulting in 3,000 chronic liver disease deaths per year
Anti-HBc Viral Markers HBV DNA HBsAg Anti-HBs Level of Detection 1 2 3 4 5 6 7 8 Months After Exposure Acute HBV Infection With Recovery
Anti-HBc Viral Markers HBV DNA HBsAg Level of Detection 1 5 6 7 8 2 3 4 Months After Exposure Chronic HBV Infection
Plasma for Further Manufacture • Both Source Plasma and recovered plasma are used for further manufacture (“fractionated”) into plasma-derived products, such as albumin, immunoglobulins, clotting factors and alpha-1 proteinase inhibitor. • During the fractionation process, plasma is pooled, purified and processed to extract plasma proteins. • These proteins are used to treat various medical diseases including hemophilia, primary immunodeficiencies and alpha-1 antitrypsin deficiencies, and acute conditions such as burns and shock.
Source Plasma • In 2008, 18.8 million Source Plasma units were donated in the U.S. • Source Plasma is collected by plasmapheresis – donor’s Whole Blood is separated into red blood cells and other cellular components that are returned to the donor and the fluid portion is collected. • Donors may donate up to twice a week with a minimum two-day period in between donations. • Donors are generally compensated.
Testing of Source Plasma • All Source Plasma for further manufacture must be tested for evidence of infection due to specific communicable disease agents including HBV (21 CFR 610.40). Currently, for HBV, Source Plasma is only tested for HBsAg. • FDA does not currently recommend that Source Plasma donations be tested for anti-HBc. • HBV NAT is currently voluntarily performed on most, if not all, Source Plasma.
Source Plasma – Voluntary Standards • Plasma Protein Therapeutics Association (PPTA) represents U.S. and European Source Plasma collectors and manufacturers of plasma-derived therapies and establishes voluntary standards for Source Plasma. • “Qualified Donor” Program • 60-day Inventory Hold • HBV NAT – (required for QSEAL certification)
Safety of Plasma Derivatives • There have been no reports of transmission of HBV to recipients of plasma derivatives since the late 1980s. • Viral inactivation and removal steps are very effective especially for enveloped viruses like HBV. • Heat inactivation (60oC for 10 hours) • Solvent detergent treatment • Nanofiltration
Safety of Plasma Derivatives (cont’d) • FDA requires at least two orthogonal (independently effective) viral clearance steps to attain an acceptable margin of safety. • The manufacturing process for plasma-derived product must be validated for its capacity to clear both enveloped and non-enveloped viruses. The total log reduction for enveloped viruses, such as HBV, should be at least 10 logs10.
HBV NAT Assays Licensed for Screening Source Plasma Donations • COBAS AmpliScreen HBV Test (Roche Molecular Systems, Inc.) for HBV with a pool size of <96 donations. • Procleix Ultrio Assay (Gen-Probe, Inc.). Multiplex assay for HIV-1, HCV and HBV with a pool size of <16 donations. • COBAS TaqScreen MPX Test. (Roche Molecular Systems, Inc.) Multiplex assay for HIV, HCV, HBV with a pool size of <96 donations.
HBV NAT Assays in Development for Screening Source Plasma Donations 1. UltraQual HBV PCR Assay (National Genetics Institute) for HBV with a pool size of <512 donations. 2. Hepatitis B Virus Deoxyribonucleic Acid, Polymerase Chain Reaction, Test (HBV DNA, PCR, NAT)(Human Plasma)(HIQ-PCR, Baxter) (BioLife Plasma Services, L.P.) for HBV with a pool size of <512 donations.
1) HBV NAT Interdiction of Potentially Infectious Source Plasma Units • Depending on the sensitivities of the assays, HBV NAT may interdict potentially infectious Source Plasma collections containing HBV DNA that are negative for HBsAg. • These units would not be detected by serology testing and would enter manufacturing pools. • These HBV NAT positive/HBsAg negative units are referred to as “yield cases.”
Summary of “Yield Cases”* (HBV NAT+/HBsAg-) Detected in Clinical Trials *includes presumptive and confirmed cases/**preliminary data
Effect of 60-Day Inventory Hold on Benefit of “Yield Cases” • Source Plasma donors typically donate twice weekly for several weeks at a time. • Therefore, if a donor seroconverts to HBsAg positive after several HBsAg negative donations, a 60-day inventory hold for Source Plasma collections would prevent some HBsAg negative units that are potentially infectious that may be HBV NAT positive from entering manufacturing pools. • The benefit of “yield case” detection by HBV NAT is potentially mitigated by the 60-day hold.
2) HBV NAT Reduction of the “Window Period” and Impact on Public Health • The “Window Period” is the period when a donor is infected with HBV but prior to the appearance of detectable HBsAg. • HBV DNA is the first marker to appear in plasma during HBV infection. • HBsAg appears an average of 6-8 weeks after exposure and declines to undetectable levels within 4-6 months if the infection is resolved.
Viral Markers HBV DNA HBsAg Window Period Level of Detection 1 2 3 4 5 6 7 8 Months After Exposure Acute HBV Infection With Recovery
Window Period • The three licensed HBV NAT tests were able to detect HBV DNA from 0-40 days earlier than HBsAg using sensitive HBsAg assays.* * Using dilutions to simulate maximum Source Plasma test pool size permitted
Window Period(cont’d) • Interdiction of potentially infectious HBV NAT positive/HBsAg negative Window Period cases may enhance the safety of plasma derivatives by removing units contaminated with HBV from further manufacture and lowering the viral titer of fractionation pools. • Donor screening by HBV NAT also permits earlier detection of HBV infection in the donor resulting in earlier notification, follow-up and medical intervention and prevention of secondary transmission to donor contacts.
3) Improved Analytical Sensitivity of HBV NAT Over HBsAg for Detection of HBV • The Limit of Detection (LOD) at the assay cutoff (50% detection rate) for PRISM HBsAg is estimated to be 1664 copies/mL* compared to 336 copies/mL for an HBV NAT assay.** **(NGI-investigational/individual sample in a pool of 512) • Estimated five-fold improvement in analytical sensitivity of donor screening for HBV • Based on the increased sensitivity of donor screening, HBV NAT is expected to lower the maximum viral titer in a plasma fractionation pool by an estimated factor of five (0.7 log10). * Kuhns, MC and Busch MP. Mol Drug Ther 2006
4) Detection of Collections During the Post- Antigenemia Recovery Phase of Acute Infections • HBsAg declines to undetectable levels within 4-6 months in the recovery phase of acute HBV infection. • HBsAg may be undetectable, but virus is still present for a brief time (1-2 weeks), i.e., unit is HBV NAT positive. • Anti-HBc is present, but not tested for Source Plasma.
Anti-HBc – not tested for Source Plasma Viral Markers HBV DNA HBsAg Window Period Second “Window Period” - Post-Antigenemia Anti-HBs Level of Detection 1 2 3 4 5 6 7 8 Months After Exposure Acute HBV Infection With Recovery
4) Detection of Possibly Infectious Collections in Occult Chronic HBV Infections • In chronic HBV infection, HBsAg is almost always positive, but HBV NAT may detect HBV DNA in a very small number of asymptomatic chronically infected individuals with undetectable HBsAg.
Impact on Public Health from Detection of HBV NAT Positive/HBsAg Negative Donations • Earlier donor notification allowing for counseling and medical treatment • Donor deferral • Prevention of secondary transmission of HBV infection to contacts
HBV NAT Assay Analytical Sensitivities and Proposed Sensitivity Standard
Analytical Sensitivity and Limit of Detection (LOD) at 95% for HBV NAT Assays *International units = IU/**preliminary data
Sensitivity Standard for HBV NAT • Detection of HBV DNA at a sensitivity of at least 500 IU/mL (95% detection rate) for the individual donation in a Source Plasma minipool may represent a reasonable and attainable standard for HBV NAT assays with added sensitivity compared to HBsAg.
Questions for the Committee 1. Do the available scientific data support the concept that testing of Source Plasma donations by HBV NAT increases the safety margin of plasma derivatives? 2. If so, is a sensitivity of at least 500 IU/mL for the individual Source Plasma collection suitable for HBV NAT when testing minipools of Source Plasma? 3. Please comment on whether detection of HBV infection in Source Plasma donors by HBV NAT adds benefit to public health compared with testing only for HBsAg.
Safety of Source Plasma for Further Manufacture • Source Plasma for further manufacture of plasma derivatives is safe with current standards. • HBV NAT would marginally increase the safety for fractionated products. • HBV NAT would have a secondary public health benefit for Source Plasma donors and their contacts.
Summary – HBV NAT for Source Plasma May enhance the margin of safety of plasma derivatives: • Interdiction of “yield cases” (HBV NAT positive/HBsAg negative) with observed yield rates of approximately 1:9,000 to 1:35,000 • Closure of the Window Period (Donor is infected with HBV but does not yet have detectable HBsAg.) • Estimated five-fold improvement in analytical sensitivity over HBsAg with lowering of the maximum viral titer in a plasma fractionation pool by an estimated factor of five (0.7 log10)
Summary – HBV NAT for Source Plasma (cont’d) May improve public health: • Earlier donor notification based on both HBV NAT and serology test results • Earlier counseling and access to medical treatment • Prevention of secondary transmission of HBV infection to contacts
Questions for the Committee 1. Do the available scientific data support the concept that testing of Source Plasma donations by HBV NAT increases the safety margin of plasma derivatives? 2. If so, is a sensitivity of at least 500 IU/mL for the individual Source Plasma collection suitable for HBV NAT when testing minipools of Source Plasma? 3. Please comment on whether detection of HBV infection in Source Plasma donors by HBV NAT adds benefit to public health compared with testing only for HBsAg.