Download
1 / 32
320 likes | 402 Vues
Dive into the spectrum of neurodegenerative dementia with a comprehensive overview of cognitive domains, diagnostic criteria, gene/biomarker testing, and treatment options. Explore the latest research in Alzheimer's Disease, MCI, and other related conditions.

E N D
The Spectrum of Neurodegenerative Dementia Russell Swerdlow, MD
NINCDS-ADRDA Criteria • Objective dementia • At least two defective cognitive domains • Progressive worsening • Normal consciousness • No other potential causes apparent *From McKhann et al, Neurology 34, 939-944.
Cognitive Domains • Judgment and Reasoning • Attention and concentration • Praxis • Executive • Language • Visuospatial • Memory
Memory Attention Working memory/Attention/ Executive Functioning Memory Language/Executive Function/ Praxis Visuospatial Function
Other Studies • Brain imaging • CT or MRI • Blood tests • CBC, chemistries, LFTs, B12, thyroid
Gene and Biomarker Testing • May help increase certainty of diagnosis • May decrease certainty of diagnosis • May help predict MCI-to-AD conversion • Being developed to facilitate/refine early dx • These efforts are primarily for research purposes
Available Gene/Biomarker Tests • Genetic Testing • FDG PET • CSF • Amyloid PET
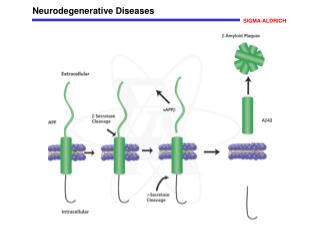
AD Biomarker “Definitions” • “Upstream” Biomarkers • CSF Abeta • Brain amyloid imaging by amyloid PET • “Downstream” Biomarkers • Tau or phospho-tau • FDG PET • MRI
2011 AD Criteria • Probable AD Dementia • Meets clinical AD criteria • No alternate diagnosis • Documented decline, biomarker, or mutation • Possible AD Dementia • Meets clinical AD criteria, BUT • Atypical course (lacks clear progression) OR • Biomarkers are negative OR • Mixed presentation (criteria for other cause also met)
2011 MCI Clinical Criteria • Concern regarding a change in cognition • By patient, informant, or clinician • Impairment in 1 or more cognitive domains • Typically 1-1.5 SD below expected • Preserved independence in functional abilities • Mild problems allowed, but essentially independent • Not demented • No evidence of social or occupational impairment
2011 MCI Criteria: Types of MCI • MCI of a Neurodegenerative Etiology • Meets MCI clinical criteria, BUT • Biomarkers not tested, OR • Biomarkers tested but are ambiguous for AD, OR • Biomarkers tested but are negative for AD • MCI of the Alzheimer Type • Meets MCI clinical criteria, AND • At least 1 AD “downstream” biomarker is present • Prodromal Alzheimer’s Dementia • Meets MCI clinical criteria, AND • There is “upstream” AD biomarker evidence
2011 Preclinical AD Criteria • Stage 1 (Asymptomatic Cerebral Amyloidosis) • Abnormal “upstream” biomarker • Normal cognition • Stage 2 (Amyloidosis+Degeneration) • Abnormal “upstream” biomarker • Abnormal “downstream” marker • Normal cognition or slight decline • Stage 3 (Amyloidosis+Degeneration+CognitiveChange) • Abnormal “upstream” biomarker • Abnormal “downstream” biomarker • Longitudinal evidence of subtle cognitive decline
(A) (B) 100 40 with clinical AD (between 30-50%) 100 90 60 80 70 60 Percent Effected (+Standard Deviation) 50 20 with MCI* (between 10-30%) 40 30 20 40 10 0 Clinical AD Clinical AD + MCI Clinical AD + MCI + Preclinical AD 25 with preclinical AD (~65% of those with no cognitive decline) 15 with no AD
AD Treatments • Cholinesterase inhibitors • Memantine • Axona • Dietary Supplements • Amyloid Treatments
FTD: Clinical Criteria • Acquired behavioral or cognitive deficits of • personality, with inappropriate activities, or • progressive language change -problems with expression -problems with word meaning/naming • Decline causes social/occupational dysfunction • Insidious and progressive • Degenerative in nature (no other etiology) • Not delirious • Not due to psychiatric disturbance McKhann et al, Arch Neurol 2001;58:1803-1809
Primary Progressive Aphasia • Inclusion Criteria (all required) • Language main clinical feature • Language main cause of ADL problems • Problems started with language • Exclusion Criteria (all required) • Other medical disorder is more likely • Psychiatric disorder is more likely • Other cognitive domains initially perturbed • Prominent initial behavioral disturbances
Non-Fluent/Agrammatic Variant PPA • At least 1 of 3 core features • Agrammatism • Effortful, halting speech; apraxia of speech • At least 2 of 3 • Impaired comp. of syntactically complex sentences • Spared single word comprehension • Spared object knowledge • Imaging Support • Left posterior frontal-insular atrophy • Left posterior frontal-insular hypometabolism
Semantic Variant PPA • Both core features present • Impaired confrontation naming • Impaired single word comprehension • At least 3 present • Impaired object knowledge • Surface dyslexia or dysgraphia • Spared repetition • Spared speech production • Imaging Support • Predominant anterior temporal lobe atrophy • Predominant anterior temporal lobe hypometabolism
Logopenic Variant PPA • Both core features present • Impaired single word retrieval • Impaired repetition • At least 3 features present • Errors in spontaneous speech and naming • Spared single word comp./object knowledge • Spared motor speech • Absence of frank agrammatism • Imaging support • Left posterior perisylvian/parietal atrophy • Left posterior perisylvian/parietal hypometabolism
PPA Etiology Predictions • Non-fluent/agrammatic • Most often tau-postitive • FTLD spectrum (may evolve into CBD or PSP) • If familial, consider checking MAPT gene; also PGRN gene • Semantic • Most often TDP • FTLD spectrum • If familial, consider checking PGRN gene • Logopenic • Most often AD pathology • Could consider checking for AD biomarkers
Behavioral Variant FTD Criteria • Progressive deterioration of behavior/cognition • Possible bvFTD (need 3 of 6) • Disinhibition (lost social skills, manners, impulsive) • Apathy or inertia • Lost sympathy or empathy • Stereotyped or compulsive/ritualistic behaviors • Hyperorality/dietary changes • NP with executive >memory and VP dysfunction • Probable bvFTD • Meets possible bvFTD criteria • Exhibits significant functioanldecelin • Imaging c/w bvFTD (frontal/anterior temporal atrophy or hypomet.)
bvFTD • Biggest recent finding: • C9ORF72 • Familial and sporadic cases reported • Especially prevalant in familial FTD-MND
Dementia with Lewy Bodies • Central feature • Progressive dementia • Core features (2 for probable, 1 for possible) • Fluctuating cognition/variable attention+alertness • Recurrent visual hallucinations • Spontaneous features of parkinsonism • Suggestive features (almost equal weight) • REM sleep behavior disorder • Severe neuroleptic sensitivity • Low dopamine transporter uptake in BG • Supportive features • Falls, LOC, autonomic dysfunction, delusions
Temporal Sequence • DLB: dementia before or with parkinsonism • PDD: dementia evolves after PD established
Pre-Mortem DLB vs. AD • Dopamine transporter (DAT) imaging • Metaiodobenzyl guanidine (MIBG) scintigraphy • FDG PET (occipital hypometabolism) • Relative hippocampal sparing on MRI
Post Mortem DLB vs. AD • 60% of time AD and LB pathology co-exist
Cogniform Disorder • Complaints/performance issues excessive (need 2 of 9) • Mild-mod injury with deficits worse than expected • Inconsistencies between complaints, deficits, injury • Inconsistencies between deficits and observed state • Temporal course not typical of that expected • Inconsistencies across multiple evaluations • Strange patterns on cog testing • Inconsistencies in sx or complaints over time • Issues with specific Validity tests (e.g. testing of effort) • Issues with parts of other tests that inform Validity • Deficits play out in everyday life • In addition to excessive complaints/poor testing on eval, sx pervade daily function (“sick role”) • Specify if: • Evidence of external incentive, interpersonal incentive, or NOS
Parahippo. Gyrus Hippocampus Entorhinal Cortex MEMORY CIRCUIT Dorsolateral Prefrontal Area (Brodmann’s 9 and 10) Glu Dorsolateral Head of Caudate Dorsolateral- Prefrontal Pathway (memory activation and search functions) GABA GPe GABA GABA STN Glu Medial Temporal Lobe Lateral Dorsomedial GPi; SNR GABA VA and DM Thalamus Medial Temporal-Thalamic Circuit (memory storage)
References • AD • McKhann GM, Knopman DS, Chertkow H, et al. The diagnosis of dementia due to Alzheimer's disease: Recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement 2011;7:263-269. • Albert MS, Dekosky ST, Dickson D, et al. The diagnosis of mild cognitive impairment due to Alzheimer's disease: Recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement 2011;7:270-279. • Sperling RA, Aisen PS, Beckett LA, et al. Toward defining the preclinical stages of Alzheimer's disease: Recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement 2011;7:280-292. • PPA • Gorno-Tempini ML, Hillis AE, Weintraub S, et al. Classification of primary progressive aphasia and its variants. Neurology 2011;76:1006-1014. • bvFTD • Rascovsky K, Hodges JR, Knopman D, et al. Sensitivity of revised diagnostic criteria for the behavioural variant of frontotemporal dementia. Brain 2011;134:2456-2477. • DLB • McKeith IG, Dickson DW, Lowe J, et al. Diagnosis and management of dementia with Lewy bodies: third report of the DLB Consortium. Neurology 2005;65:1863-1872. • Cogniform Disorder • Delis DC, Wetter SR. Cogniform Disorder and Cogniform Condition: proposed diagnoses for excessive cognitive symptoms. Arch ClinNeuropsychol 2007;22:589-604.