Download
1 / 55
610 likes | 1.02k Vues
FNA of the Thyroid. Lisa Kendrick BSc., RT Cytology, CT (ASCP) School of Diagnostic Cytology Health Sciences Centre. Objectives . Describe the anatomy of the thyroid. Describe the histologic features of the thyroid List and describe the normal cytologic features of the thyroid.

E N D
FNA of the Thyroid Lisa Kendrick BSc., RT Cytology, CT (ASCP) School of Diagnostic Cytology Health Sciences Centre
Objectives • Describe the anatomy of the thyroid. • Describe the histologic features of the thyroid • List and describe the normal cytologic features of the thyroid. • State the requirement of adequacy for a FNA of the thyroid. • List and describe the common benign conditions of the thyroid. • List and describe the common malignancies of the thyroid. • List and describe the common metastatic malignancies of the thyroid. • Discuss the various methods of treatment of malignancies of the thyroid.
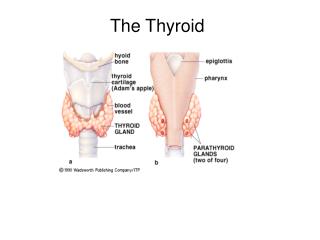
Anatomy • Located below the larynx • Consists of two lobes that lie on either side of the trachea • Lobes are connected by an ithmus • Is an endocrine gland • Concepts of Human Anatomy and Physiology, Van de Graff and Fox, page 504, Figure 19.13
Histology • Consists of spherical sacs – thyroid follicles • Lined by simple cuboidal epithelium • Contains colloid • Wheater’s Functional Histology 3rd Edition, Burkitt, Young and Heath, page 310, Figure 17.7
Follicular Cells • Nucleus • Central • Round/oval • Finely granular chromatin • 1 – 2 nucleoli • Cytoplasm • Pale • Indistinct • Arrangement • Honeycomb pattern
Hurthle Cells • AKA Askanazy cells or Oncocytes • Large, polygonal cells • Nucleus • Round/oval • Eccentric • Finely granular chromatin • Cytoplasm • Abundant • Granular • Eosinophilic
Colloid • Found in the background • May stain blue, pink or metachromatic • Two states: • Watery Thick
Satisfactory Specimen • 5 or more groups of 10 cells each on a minimum of 2 slides
Colloid Nodule • Most common form of goiter in adolescents and young women • Follicular cells cease to proliferate and colloid accumulates within the follicles
Colloid Nodule • Cytology • Macrofollicular pattern • Variable cellularity • Hurthle cell change may be seen • Scant follicular cells (normal in appearance) • Macrophages • Abundant colloid
Cystic Degeneration • FNA can cure 20 – 60% of cystic lesions by evacuation • Cytology • Few follicular cells • Abundant macrophages
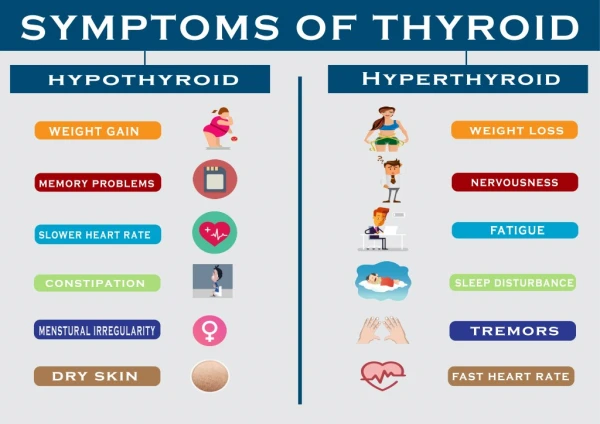
Hashimoto’s Thyroiditis • AKA chronic thyroiditis • An autoimmune disorder • Affects women more than men • Associated with hyperthyroidism
Hashimoto’s Thyroiditis Cytology • Cellular aspirate presenting in small groups, fragments • Groups of Hurthle cells • Follicular cells with Hurthle cell change • Inflammatory cells (lymphocytes and macrophages) • Tingible body macrophages • Little colloid • Possible lymphoma association
Follicular Carcinoma • Peak onset ages 40 through 60 • Females more common than males by 3 to 1 ratio • Prognosis directly related to tumor size [less than 1.0 cm (3/8 inch) good prognosis] • Rarely associated with radiation exposure • Spread to lymph nodes is uncommon (~10%) • Invasion into vascular structures (veins and arteries) within the thyroid gland is common • Distant spread (to lungs or bones) is uncommon, but more common than with papillary cancer • Overall cure rate high (near 95% for small lesions in young patients), decreases with advanced age • www.endocrineweb.com/capap.html
Follicular Carcinoma • Distinction between neoplasm and carcinoma depends on the histology specimen • Identification of invasion of either the capsule or blood vessels confirms the diagnosis of carcinoma • It is very difficult to differentiate between neoplasm and carcinoma based on morphology alone
Follicular Neoplasms • The cellularity varies • No colloid • Cells are arranged in small, loosely cohesive groups • Micro follicular pattern is observed • Syncytial patterns predominate • There may be overlap of some features with a colloid nodule
Follicular Neoplasm • Nucleus • Round • Smooth membrane • Fine/coarse even chromatin • Macronucleoli • Cytoplasm • Pale • Poorly defined
Papillary Carcinoma • Peak onset ages 30 through 50 • Females more common than males by 3 to 1 ratio • Prognosis directly related to tumor size [less than 1.5 cm (1/2 inch) good prognosis] • Accounts for 85% of thyroid cancers due to radiation exposure • Spread to lymph nodes of the neck present in more than 50% of cases • Distant spread (to lungs or bones) is very uncommon • Overall cure rate very high (near 100% for small lesions in young patients) • www.endocrineweb.com/capap.html
Papillary Carcinoma • Highly variable cellularity (very cellular to scant or cystic) • Little to no colloid • Papillary arrangements or monolayered fragments • Syncytia may be present • Enlarged polygonal cells
Papillary Carcinoma • Nucleus • Central • Overlapping • Round/oval/pleomorphic/ angulated • Finely granular (powdery) chromatin • Micro or macro nucleoli • Folds and creases (grooves) • Cytoplasmic nuclear inclusions • Abundant cytoplasm • Psammoma bodies may be present • Multinucleated macrophages
Hurthle Cell Neoplasm • Cellularity varies • Little to no colloid • Cells are dispersed or arranged in loose monolayers • May be follicular growth pattern • Monomorphic population of Hurthle cells • May have red macronucleoli • May demonstrate binucleation • May demonstrate nuclear grooving
Hurthle Cell Neoplasm • There is no clear separation between adenomas and carcinoma • However if the following features are present a carcinoma may be suspected: • Hypercellularity • Syncytia • Increased N:C • Nuclear pleomorphism • Multinucleoli
Medullary Carcinoma • Occurs in 4 clinical settings and can be associated with other endocrine tumors • Females more common than males (except for inherited cancers) • Regional metastases (spread to neck lymph nodes) occurs early in the disease • Spread to distant organs (metastasis) occurs late and can be to the liver, bone, brain, and adrenal medulla • Not associated with radiation exposure • Usually originates in the upper central lobe of the thyroid • Poor prognostic factors include age >50, male, distant spread (metastases), and when seen in patients with other endocrine tumors due to MEN II-B syndrome. • Residual disease (following surgery) or recurrence can be detected by measuring calcitonin (a hormone that should be measured every 4 months for the first few years and then every 6 months for ever). • www.endocrineweb.com/capap.html
4 Variants • Sporadic • MEN II-A (Sipple Syndrome) • MEN II-B • Inherited Medullary Carcinoma
Medullary Carcinoma • Not a common malignancy • Can be multifocal (in which the clinician may remove the entire thyroid) • Lymph node involvement is common
Medullary Carcinoma • Cellularity varies • Cell morphology varies • Plasmacytoid • Round • Polygonal • Spindle • Arranged in loose groups • Single cells are common • Amyloid may be present in the background
Medullary Carcinoma • Nuclei • Oval/pleomorphic • Coarse salt and pepper chromatin pattern • Central or eccentrically located • Indistinct nucleoli • Binucleation may be seen • Intranuclear inclusions may be seen • Cytoplasm is finely granular
Anaplastic Carcinoma • Very rare • Diagnosis is often suggested by clinical findings
Peak onset age 65 and older • Very rare in young patients • Females more common than in males • Typically presents as rapidly growing neck mass • Can occur many years after radiation exposure • Spread to lymph nodes of the neck present in more than 90% of cases • Distant spread (to lungs or bones) is very common even when first diagnosed • Overall cure rate very low • Typically requires a very aggressive treatment plan with surgery, radiation and sometimes even chemotherapy. • Often requires the patient to get a tracheostomy to maintain their airway. • www.endocrineweb.com/capap.html
Anaplastic Carcinoma • Giant or mixed forms • Variable cellularity • Inflammatory cells and necrotic debris are found in the background • Variable cell morphology • Squamoid • Giant cell • Spindle cell
Anaplastic Carcinoma • Nucleus • Pleomorphic in shape • Irregular membrane • Coarse, irregularly distributed chromatin • Prominent nucleoli • Atypical mitosis • Multinucleation • Cytoplasm • Densely granular
Metastatic Malignancies • Thyroid is a common site for metastases • Common metastatic tumors include: • Adenocarcinoma of the breast • Renal cell carcinoma • Squamous cell carcinoma from elsewhere • Melanoma • Lymphoma
Metastatic Melanoma • Cells are very pleomorphic • Pigment is often not present • Clinical history is very important • Immunohistochemistry aids in the diagnosis (S100, HMB45)
Lymphoma • Non-Hodgkin’s Hodgkin’s • monotonous population - Lymphoid cells and of lymphoid cells Reed-Sternberg cells
Surgery • Two types • 1. Lobectomy • The entire thyroid is removed. • 2. Hemithyroidectomy (lobectomy): • The surgeon removes the entire lobe on the side of the thyroid where the growth or cancer is found. If a biopsy of the growth confirms cancer, the surgeon may also remove the other lobe.
Radiation Therapy • Three types of radiation therapy: • 1. External beam radiation therapy - In external beam radiation therapy, radiation is directed at the cancer and surrounding tissue from a machine outside the body. It is used to treat most types of cancer. • 2. Brachytherapy - treats the cancer with a high total dose of radiation in a concentrated area in a short period of time. Sealed radioactive sources are placed in the body, in or near the cancer. A sealed radioactive source is often called an implant. • 3. Systemic radiation therapy - the radiation source is given as a liquid (either as a drink or in capsules that are swallowed) or by injecting it into a vein (an intravenous injection). The radiation source travels throughout the body.
Radioactive Iodine Therapy (RAI) • Radioactive iodine (also called iodine-131 or I-131) is commonly used to treat thyroid cancer. It is given either as a drink or as a capsule. Thyroid cells and cancer cells absorb the radioactive iodine. It destroys any cancer cells and normal thyroid cells that may still be in the body after surgery. • After radioactive iodine therapy, thyroid hormone replacement therapy is required to replace the hormone that was made by the thyroid cells.
Thyroid Hormone Treatment • Thyroid hormone therapy is sometimes used to treat papillary or follicular thyroid cancer. It is given as pills. The hormone thyroxine (T4) slows the growth of thyroid cancer cells that may be left in the body after surgery.