Understanding Glomerular Diseases: Pathological Features and Presentations
640 likes | 826 Vues
Learn about glomerular diseases based on pathological features and presentations like proteinuria, hematuria, salt retention, and renal impairment. Explore glomerular syndromes and their diagnosis, treatment, and prognosis.

Understanding Glomerular Diseases: Pathological Features and Presentations
E N D
Presentation Transcript
** Pathological features: • Diagnosis of glomerular diseases based on pathological features • Focal: some but not all the glomeruli contain the lesion. • Diffuse: global, most, more than 75% of the glomeruli contain the lesion.
3. Segmental: only part of the glomerulus is affected ((most of the focal lesions are also segmental)) 4. Proliferation: Increase in the cell number with or without inflammatory cell infiltration. 5. Membrane alteration: capillary wall thickening or basement membrane alteration.
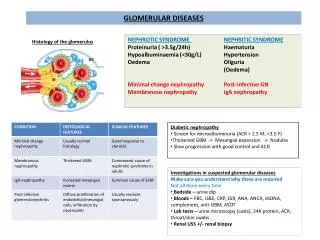
** Presentations: • Protienuria: Which is due to either: a. loss of the net negative charge on the capillary wall (( selective protienuria )) b. structural defect in the filtration barrier (( non selective protienuria )) * when protienuria exceed 3.5 gm/day it is called (( Nephrotic range protienuria ))
2. Haematuria: in form of dysmorphic RBC and RBC casts. 3. Salt retention: may expressed as oedema, volume overload, hypertension & congestive heart failure. 4. Renal impairment: ranging from minimal to severe impairment requiring dialysis.
****NEPHRETIC SYNDROME: This syndrome is characterized by the abrupt onset (( days )) of haematuria with RBC cast and protienuria less than 3.5 gm/day, temporally associated with hypertension and renal impairment.
1.POSTSTREPTOCOCCAL GN: It is a complication for certain strains of group A, β-hemolytic streptococci. Usually with 5 – 20 days latent period, typically in children 3 – 12 years but it can occur in adult.
The patient presented with malaise, cola colored urine, haematuria, mild hypertension, periorbital oedema, protienuria and renal impairment (variable ).
Investigations: • Haematuria, RBC cast • Protienuria < 3.5 gm/day. • High ASO titer • Low serum complement
Treatment: • Non specific treatment • Salt restriction • Diuretics • Antihypertensive • Antibiotics, if culture positive for streptococci • Dialysis in cases of severe acute renal failure
Prognosis: • Complete recovery in 90% • Rarely progress to CRF mainly older age and oliguria > 7 days.
2. Non Streptococcal postinfectious GN: • Bacterial: Staphylococci, Pneumococci • Viral : Mumps, Coxsackie, Varicella • Protozoal: Toxoplasmosis • Usually same presentation to PSGN with low serum complement and evidence of the underlying infection itself.
3. GN associated with infective endocarditis: *Commonly with chronic right side cardiac involvement, *mild presentation, * low serum complement, *Treated by treatment of the underlying cause.
4.SHUNT NEPHERITIS : Low serum complement 5. GN associated with visceral abscesses: • Mostly with pulmonary abscesses, normal complement, successful antibiotic therapy result in recovery in renal function only in about 50% of patients.
***** RAPIDLY PROGRESSIVE GN • It characterized by nephronal haematuria with renal failure developing over weeks to months and diffuse glomerular crescent formation on renal biopsy
1. Anti – Glomerular Basement membrane GN: • eg. GOOD PASTURE’S SYNDROME: It is a disorder that affect young male more than female. Usually presented with hemoptysis, dyspnea, pulmonary hemorrhage and normal serum C3 level. Treatment with high dose steroid and plasma exchange.
2.IMMUNE COMPLEX RPGN: • Almost always associated with underlying disease • The prognosis of the underlying condition decline in the presence of immune complex RPGN.
3. NON IMMUNE MEDIATED RPGN: • It is seen in association with one of systemic vasculitis such as polyarteritis nodosa or as an idiopathic form. • Treatment by; Steroid, Plasma exchange & Cytotoxic.
1. Isolated protienuria • Asymptomatic, less than 2gm/ day. • Postural protienuria • May represent early manifestation of more serious glomerular disease eg. Diabetic nephropathy • May accompany other conditions eg. Febrile illness, congestive heart failure or infectious diseases.
2. Isolated haematuria with or without protienuria: It could be represent early manifestation of another glomerular disease such as SLE, but it may be the primary presentation of:
A. Ig A Nephropathy: • It is the most common primary glomerular disease • The typical presentation is gross haematuria following viral infection • Male > female • Age 15 – 35 years • Mild protienuria.
Normal serum complement • Progressive renal impairment may developed after 20 years. • No effective therapy • Poor prognostic indicators include: hypertension & heavy protienuria
B. ALPORT’S SYNDROME: • Hereditary disease, X – linked. • Presented in childhood with recurrent gross haematuria, mild protienuria and sensorineural deafness. • Often develop renal failure by the age of 30 years. • No effective treatment.
C. THIN BASEMENT MEMBRANE DISEASE: • It affect both genders • Usually presented with haematuria without protienuria in asymptomatic young adult. • Excellent prognosis.
D. Benign Recurrent Haematuria: • It is diagnosed by asymptomatic haematuria when other possibilities are excluded. • May presented with gross haematuria associated with febrile illness, exercise or immunization. • Renal biopsy is normal in most of them. • The overall prognosis is excellent.
NEPHROTIC SYNDROME • It characterized by the presence of: • Protienuria more than 3.5 gm/day. • Hypoalbuminemia • Oedema • Hyperlipidemia
Nephrotic Syndrome with bland sediment (( pure Nephrotic )) A. Primary Glomerular Disease: 1. Minimal Change Nephrotic Syndrome: (( MCNS )): 2. FOCAL SEGMENTAL GLOMERULOSCLEROSIS (( FSGS )): 3. MEMBRANOUS GLOMERULOPATHY B. SECONDARY GLOMERULAR DISIEASES
1. Minimal Change Nephrotic Syndrome: (( MCNS )): • Sudden onset, commonly in children aged 2 – 6 years. • Less in adulthood
*Upper respiratory tract infection may precedes the onset of the disease *Some adult with Hodgkin’s disease developed MCNS. *They are usually normotensive.
INVESTIGATIONS: • Typical Nephrotic Syndrome • No active sediment in the urine (( No RBC & Cast )). • Normal renal function
Normal serum complement • Renal biopsy : normal light microscopy but the electron microscopy shows fusion of the foot processes.
TREATMENT: Predenselon 1 – 2 mg/kg/day for 4 weeks then 1 mg/kg/day on alternative days for 4 weeks with tapering over the next 4 – 6 months .
Those with frequent relapses &/or steroid dependent may get benefit from adjective therapy with Cytotoxic alkylating agents.
2. FOCAL SEGMENTAL GLOMERULOSCLEROSIS (( FSGS )): • More in adult • Presented with heavy protienuria • Hypertension and renal impairment are common
Serum complement levels are normal. • FSGS may developed in patients with AIDS, Reflux nephropathy & Heroin abusers.
minority respond to steroid therapy, majority progress to CRF, the reminder follow a long term courses with relapses and remissions.
3. MEMBRANOUS GLOMERULOPATHY: • Mostly in adult • Normal serum complement • The majority are idiopathic but can be associated with Syphilis, hepatitis B, Ca- stomach, Ca-lung and drugs eg. Captoprill.
* Usually follow slowly progressive course * Alternated days of steroid regimen may reduce the development of CRF. *Cytotoxic agents effect is uncertain.
1. DIABETIC NEPHROPATHY: 2. AMYLOIDOSIS: B. SECONDARY GLOMERULAR DISIEASES:
1. DIABETIC NEPHROPATHY: • 5 years or more of insulin dependence have passed. • Clinically apparent usually 15 – 20 years after diagnosis of DM
Initially the protienuria is minimal and transient so it is called microscopic albuminuria but it will progress to constant moderate to severe protienuria within 2 years. Once protienuria become constant, a rapid decline in GFR begins with resultant ESRF within 5 years.
Hypertension accompany 50% of diabetic nephropathy. • More than 90% of patients with diabetic nephropathy have also retinopathy while only 1/3 of those with retinopathy have nephropathy.
A non diabetic aetiology suggested in the absence of retinopathy, diabetes duration less than 10 years and presence of microscopical haematuria with or without RBC cast.
ESRF associated with boats of hypoglycemia. • Good glycemic control prevent early diabetic microangiopathy • Antihypertensive therapy appears to slow the rate of renal deterioration
2. AMYLOIDOSIS: • Primary Amyloidosis: • Old age, usually 6th decade of life • Unexplained spleenomegaly • Enlarged tongue • Cardiomegaly • Malabsorption
2. Secondary Amyloidosis: • Younger age • Developed in patients with multiple myeloma, bronchiectasis, chronic suppuration, chronic infectious diseases and FMF.
Renal involvement is common in all forms of Amyloidosis. Protienuria may present for years prior to diagnosis. Onset of nephrotic syndrome or fall in GFR signal a rapid progression to CRF within 3 years.
DIAGNOSIS: It is confirmed by Congo – red positive tissue biopsy TREATMENT: Usually ineffective except the use of colchicine in FMF. Renal transplant has been tried.